
Abstract
Introduction
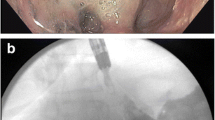
The use of self-expandable stents to treat postoperative leaks and fistula in the upper gastrointestinal (GI) tract is an established treatment for leaks of the upper GI tract. However, lumen-to-stent size discrepancies (i.e., after sleeve gastrectomy or esophageal resection) may lead to insufficient sealing of the leaks requiring further surgical intervention. This is mainly due to the relatively small diameter (≤30 mm) of commonly used commercial stents. To overcome this problem, we developed a novel partially covered stent with a shaft diameter of 36 mm and a flare diameter of 40 mm.
Methods
From September 2008 to September 2010, 11 consecutive patients with postoperative leaks were treated with the novel large diameter stent (gastrectomy, n = 5; sleeve gastrectomy, n = 2; fundoplication after esophageal perforation, n = 2; Roux-en-Y gastric bypass, n = 1; esophageal resection, n = 1). Treatment with commercially available stents (shaft/flare: 23/28 mm and 24/30 mm) had been unsuccessful in three patients before treatment with the large diameter stent. Due to dislocation, the large diameter stent was anchored in four patients (2× intraoperatively with transmural sutures, 2× endoscopically with transnasally externalized threads).
Results
Treatment was successful in 11 of 11 patients. Stent placement and removal was easy and safe. The median residence time of the stent was 24 (range, 18–41) days. Stent dislocation occurred in four cases (36 %). It was treated by anchoring the stent. Mean follow-up was 25 (range, 14–40) months. No severe complication occurred during or after intervention and no patient was dysphagic.
Conclusions
Using the novel large diameter, partially covered stent to seal leaks in the upper GI tract is safe and effective. The large diameter of the stent does not seem to injure the wall of the upper GI tract. However, stent dislocation sometimes requires anchoring of the stent with sutures or transnasally externalized threads.





Similar content being viewed by others


References
Ott C, Ratiu N, Endlicher E, Rath HC, Gelbmann CM, Scholmerich J, Kullmann F (2007) Self-expanding Polyflex plastic stents in esophageal disease: various indications, complications, and outcomes. Surg Endosc 21:889–896
Swinnen J, Eisendrath P, Rigaux J, Kahegeshe L, Lemmers A, Le MO, Deviere J (2011) Self-expandable metal stents for the treatment of benign upper GI leaks and perforations. Gastrointest Endosc 73:890–899
Fischer A, Thomusch O, Benz S, von Dobschuetz E, Baier P, Hopt UT (2006) Nonoperative treatment of 15 benign esophageal perforations with self-expandable covered metal stents. Ann Thorac Surg 81:467–472
van Boeckel PG, Sijbring A, Vleggaar FP, Siersema PD (2011) Systematic review: temporary stent placement for benign rupture or anastomotic leak of the oesophagus. Aliment Pharmacol Ther 33:1292–1301
Blackmon SH, Santora R, Schwarz P, Barroso A, Dunkin BJ (2010) Utility of removable esophageal covered self-expanding metal stents for leak and fistula management. Ann Thorac Surg 89:931–936
Tuebergen D, Rijcken E, Mennigen R, Hopkins AM, Senninger N, Bruewer M (2008) Treatment of thoracic esophageal anastomotic leaks and esophageal perforations with endoluminal stents: efficacy and current limitations. J Gastrointest Surg 12:1168–1176
Freeman RK, Ascioti AJ, Wozniak TC (2007) Postoperative esophageal leak management with the Polyflex esophageal stent. J Thorac Cardiovasc Surg 133:333–338
Edwards CA, Bui TP, Astudillo JA, de la Torre RA, Miedema BW, Ramaswamy A, Fearing NM, Ramshaw BJ, Thaler K, Scott JS (2008) Management of anastomotic leaks after Roux-en-Y bypass using self-expanding polyester stents. Surg Obes Relat Dis 4:594–599
Bege T, Emungania O, Vitton V, Ah-Soune P, Nocca D, Noel P, Bradjanian S, Berdah SV, Brunet C, Grimaud JC, Barthet M (2011) An endoscopic strategy for management of anastomotic complications from bariatric surgery: a prospective study. Gastrointest Endosc 73:238–244
Eubanks S, Edwards CA, Fearing NM, Ramaswamy A, de la Torre RA, Thaler KJ, Miedema BW, Scott JS (2008) Use of endoscopic stents to treat anastomotic complications after bariatric surgery. J Am Coll Surg 206:935–938
Low DE (2011) Diagnosis and management of anastomotic leaks after esophagectomy. J Gastrointest Surg 15:1319–1322
D’Cunha J, Rueth NM, Groth SS, Maddaus MA, Andrade RS (2011) Esophageal stents for anastomotic leaks and perforations. J Thorac Cardiovasc Surg 142:39–46
Hirdes MM, Vleggaar FP, Van der LK, Willems M, Totte ER, Siersema PD (2011) Esophageal perforation due to removal of partially covered self-expanding metal stents placed for a benign perforation or leak. Endoscopy 43:156–159
Acknowledgments
This work was funded by departmental funds of the Department of Surgery, University of Freiburg, Freiburg, Germany.
Disclosures
Drs. Ficher, Bausch, and Richter-Schrag have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fischer, A., Bausch, D. & Richter-Schrag, HJ. Use of a specially designed partially covered self-expandable metal stent (PSEMS) with a 40-mm diameter for the treatment of upper gastrointestinal suture or staple line leaks in 11 cases. Surg Endosc 27, 642–647 (2013). https://doi.org/10.1007/s00464-012-2507-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2507-x