
Abstract
Background and Purpose
Cognitive deficits that are associated with coronavirus disease 2019 (COVID-19) and occur in the acute period are gaining importance. While most studies have focused on the elderly severely affected during acute infection, it remains unclear whether mild to moderate COVID-19 results in cognitive deficits in young patients. This study aims to evaluate the post-infection cognitive functions of young adults with mild to moderate symptoms of COVID-19.
Methods
A total of 100 adults with similar age and educational background were included in the study. Half of those had been infected with COVID-19 in the last 60 days (N = 50), and the other half had not (N = 50). Global cognitive skills of the participants were evaluated through Montreal Cognitive Assessment Scale (MoCA) and Clock-Drawing Test; memory functions with Öktem Verbal Memory Processes Test (Ö-VMPT); attention span with Digit Span Test; executive functions with Fluency Tests, Stroop Test, and Trail Making Test; visual perceptual skills with Rey Osterrieth Complex Figure Test (ROCF); and neuropsychiatric status with Neuropsychiatric Inventory (NPI). Evaluations were performed in the experimental group for 21 to 60 days from the onset of the disease, and throughout the study, in the control group.
Results
It was found that global cognitive skills, verbal memory, visual memory, executive function, and neuropsychiatric status were affected during COVID-19 (p < 0.05).
Conclusion
When the cases were analyzed according to disease severity, no relationship was found between cognitive deficits and disease severity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Coronavirus disease 2019 (COVID-19) is a severe acute respiratory syndrome disease, the first cases of which appeared in Wuhan, China at the end of 2019, and which caused the death of millions of people around the world. In addition to its acute effects, it poses a threat with its long-term effects. Although it is primarily known as a respiratory disease [1], it has been stated that it may also cause neurological, psychiatric, psychological, and psychosocial disorders [2]. A study conducted in China reported that 53 (25%) of 214 patients hospitalized for the first time had central nervous system (CNS) involvement, including non-specific encephalopathy (headache, confusion, and disorientation) [3]. In a study conducted in France, it was stated that 69% of 58 hospitalized patients had CNS involvement, and 33% of 43 patients discharged from the hospital had dysexecutive syndrome including inattention, disorientation, or poorly organized response to the command [4]. A recent study carried out in England found that mental status changes including psychosis and neurocognitive changes were observed in 31% of 125 patients [1, 5]. Although the neurovirulence of the COVID-19 has not been completely proven yet, some studies showed that it affects the CNS in different ways, and causes neurological problems such as ischemia and encephalitis in two-thirds of hospitalized patients [1]. It is not known how much of the ischemic damage occurs secondary to cardiorespiratory disease through direct effects of the virus on the CNS. However, cerebral white matter affection, which is sensitive to ischemia, is stated to contribute to cognitive deficits such as attention problems, and impairments in verbal memory and executive functions [6, 7]. These findings have also been supported by the results that hippocampal damage can be observed at the cellular level after infection in studies on animals [7]. It is also stated that hypercoagulatory and hyperinflammatory states that can be observed in severe COVID-19 cases may contribute to delirium and possible cognitive deficits in the future [7].
The viral effect of COVID-19 creates, no matter how small or big it is [1, 6], a decrease in physical activity as a result of the isolation brought about by the pandemic [8, 9], and indirect effects such as loneliness [10, 11] have negative effects on the cognitive skills of individuals.
When the literature is reviewed, it is observed that due to the high rate of death and sequelae, COVID-19 studies have focused on the elderly population, and studies on the young population without serious disease have been insufficient. However, it is stated that COVID-19 might cause difficult-to-notice deteriorations in cognitive skills such as memory, attention, and concentration although they do not affect daily life [12]. For all these reasons, it is of significance to design a study that evaluates the impact of COVID-19 on younger populations in detail. To the best of our knowledge, our study is the first one conducted on a young population with no serious symptoms. This study aims to evaluate the changes in cognitive skills after infection in young individuals who suffered from COVID-19 and did not have serious symptoms.
Materials and methods
This study was ethically and scientifically approved by the Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee with the decision number E-10840098–772.02–65,171 on December 10, 2020, and was registered on ClinicalTrials.gov (NCT04978246). Oral and written consents were obtained from the participants.
Patient description
This study was conducted on 100 volunteers who were employees of Medipol Mega Hospital and students of Istanbul Medipol University between December 2020 and June 2021. These individuals with or without COVID-19 were divided into experimental (n = 50) and control group (n = 50). Criteria for inclusion in the experimental group are as follows: the patient must be between the ages of 18 and 50, they must have a positive COVID-19 RT-PCR test result, a minimum of 21 and a maximum of 60 days must pass since the test date, and the patient must have no need for oxygen supplement and mechanical ventilation or no history of hospitalization. The participants in the control group were matched according to age, gender, and education level of those in the experimental group. Those who had received treatments for cognitive dysfunctions and had been diagnosed with psychiatric disorders were excluded from the clinical study.
The severity of COVID-19 symptoms in the experimental group was classified as mild to moderate by using the WHO criteria [13]. There were no participants who were asymptomatic or diagnosed with pneumonia. No further tests (CT etc.) were required by the doctors working at the COVID-19 clinic. The pO2 level could not be measured because the general health status of the individuals in the experimental group was good, and they did not need to go to the hospital. The individuals in the control group were not previously diagnosed with COVID-19, and it was confirmed from the government’s general health system.
Study design
All participants in the experimental group were assessed in detail for 21 to 60 days from the onset of the disease. All evaluations of the control group were performed during the study, and statistical analysis of the data of both groups was carried out. The following were used for the evaluations: Global cognitive functions were evaluated via MoCA [14] and Clock-Drawing Test [15]; memory functions via Ö-VMPT [16]; attention span via Digits Forward and Backward Tests [17]; executive functions via Verbal Fluency Test [18], Stroop Test [19], and Trail Making Test A and B (TMT-A and TMT-B) [20]; visual perceptual functions via ROCF test [21, 22]; and behavioral symptoms via NPI [23]. However, the participants in the experimental group were divided into two groups in terms of symptom severity, and the relationship between cognitive deficits and disease severity was analyzed.
Statistical analysis
SPSS 22.0 for Windows was used for statistical analysis. Categorical variables are given as numbers and percentages for the descriptive statistics, and the other variables are presented as mean ± standard deviation and minimum–maximum value. The conformity of the variables to the normal distribution was checked with the Kolmogorov–Smirnov test. The Mann–Whitney U test was used to compare the results of neuropsychometric evaluations that were not in accordance with the normal distribution, and two-sample t-test was used to compare those in accordance with the normal distribution. In all tests applied to the variables, the significance level was accepted as p ≤ 0.05 and the confidence interval as 95%. The estimation of effect size was calculated with Cohen’s d. The effect size was interpreted as 0.2 low, 0.5 medium, and 0.8 large effect size [24].
Results
Demographic data of the participants in the experimental and control group are presented in Table 1. When the two groups were compared in terms of gender, age, and years of education, no significant difference was found (p > 0.05).
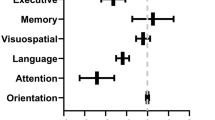
Neuropsychometric evaluation results of the experimental and control group were compared. Participants in the experimental group showed worse performances on MoCA Test (p = 0.000), Clock-Drawing Test (p = 0.004), Ö-VMPT Learning (p = 0.000), Delayed Recall (p = 0.002) and Recognition (p = 0.009) of the Ö-VMPT, Phonemic Fluency (p = 0.006) and TMT-A scores (p = 0.015), ROCF Copy (p = 0.040), Immediate Recall (p = 0.002) and Delayed Recall (p = 0.000), and Neuropsychiatric Inventory (p = 0.001). There were no significant differences between the two groups in Digits Forward and Backward Tests, Semantic Fluency, Stroop Time, Stroop Error, and TMT-B Tests (p > 0.05), but the participants in the experimental group performed worse in these tests compared to the control group. Cohen’s d was calculated to estimate an effect size and is high in MoCA and Ö-VMPT. It is moderate to small in the other tests which are significant according to p value. The details are presented in Table 2.
Comparison of neuropsychiatric characteristics, which are subparameters of NPI test, according to frequency × severity score for both groups is given in Table 3. None of the patients reported complaints of delusions, elation/euphoria, disinhibition, and aberrant motor behavior; that is why they are not included in the table. It was found that the individuals in the experimental group experienced more significant changes in apathy (p = 0.016), sleep and night-time behavior (p = 0.001), and appetite and eating changes (p = 0.005) compared to the control group. Cohen’s d is moderate to small in sleep and night-time behavior, appetite and eating changes, hallucinations, anxiety, and apathy/indifference.
Classification of the experimental group by disease severity
The experimental group was divided into two subgroups: those with mild (n = 29) and those with moderate (n = 21) COVID-19 [13]. When the two groups were compared in terms of gender, age, and years of education, no significant difference was found (p > 0.05). Demographic characteristics of the groups are given in Table 4.
Data on mild and moderate symptoms are provided in Table 5. Of the patients with mild symptoms, 20 had loss of taste and smell (28.2%), 16 had headache (22.5%), 15 had myalgia (21.2%), 8 had fatigue (27.6%), 8 had cough (27.6%), 1 had a fever (1.4%), 2 had loss of appetite (2.8%), and 1 had diarrhea (1.4%). Of the patients with moderate symptoms, 20 had loss of taste and smell (14.6%), 13 had headache (15.9%), 13 had myalgia (15.9%), 6 had fatigue (7.3%), 12 had cough (14.6%), 17 had fever (20.7%), 2 had loss of appetite (2.4%), 2 had diarrhea (2.4%), and 5 had dyspnea (6.1%).
The neuropsychometric evaluation results (MoCA, Clock-Drawing Test, Ö-VMPT Learning, Delayed Recall and Recognition, Semantic Fluency and Phonemic Fluency, Stroop Time and Stroop Error, TMT-A and TMT-B, ROCF Copy, Immediate Recall and Delayed Recall, NPI) of the groups with mild and moderate COVID-19 were compared. No significant difference was observed (p > 0.05). Cohen’s d is small in memory tests, phonemic fluency, and ROCF (Copy and Immediate Recall). The details are presented in Table 6.
The subparameters of the NPI evaluating neuropsychiatric features were compared according to the groups with mild and moderate COVID-19. There was no statistical difference between them (p > 0.05). Cohen’s d is small in depression/dysphoria, apathy/indifference, and sleep and night-time behavior. The details are given in Table 7.
Discussion
Our study investigated the status of cognitive functions after infection in adults with COVID-19 who had mild to moderate disease. We found that patients’ general cognitive skills, memory, executive functions, visual memory skills, and neuropsychiatric status were impaired. In addition, we found remarkable findings on the presence of apathy, sleep and night-time behavior disturbances, and appetite and eating abnormalities in patients with COVID-19, as well as the effect on general mood. When we compared the neuropsychometric evaluation results of the patients with mild and moderate disease, we found that there was no difference between the two groups.
Although the effect of COVID-19 on CNS is not well known [1, 25], it is stated that post-infection neurological symptoms are observed at a rate of 36.4% [3] and may cause permanent or temporary impairments in cognitive functions [26]. Many studies in the literature have noted that the global cognitive skills of individuals with COVID-19 are declining [27,28,29]. Being suspected or confirmed to have picked up COVID-19 and recovered, 84,285 individuals of various age groups, with various disease severity, comorbidities, and educational level, were assessed online in a study in the UK. The study, in which the mean age of the participants was 46, indicated that there was a decrease in the general cognitive performance of the individuals receiving treatment. Although it was stated that the results were proportional to the level of treatment, a significant decrease was found in the global cognitive performance of everyone with or without respiratory problems [27]. In another study conducted on individuals whose cognitive skills were measured before the pandemic and whose mean age was 62.6 years, it was reported that there was a 4-point decrease in MoCA scores of those who survived the disease with mild symptoms, and there were EEG findings supporting this in some cases [28]. When the literature is reviewed, it is observed that the studies are conducted in the advanced age group, and there is a decrease in the global cognitive performance of individuals with mild or severe COVID-19 [28,29,30]. Although, unlike most of the literature, this study was performed in the young population, the fact that the global skills, which we evaluated through MoCA and clock drawing, significantly decreased in individuals with COVID-19 compared to those without is in line with most studies.
Although it is stated that the neurological symptoms of COVID-19 are common, the incidence, duration, and underlying neural basis of cognitive abilities are not fully known. However, it is said that the hippocampus is particularly vulnerable to coronavirus infection, which can increase post-infection memory disorders [30,31,32,33] and accelerate degenerative diseases such as Alzheimer’s [33]. It is also underlined that memory is one of the cognitive skills most affected after COVID-19 [31]. In addition to the neural effect of infection on memory, some studies report that loneliness, which is the result of isolation during the pandemic, also affects memory skills [11]. Although the cause is not known clearly, the results of our study, in which we recorded a decrease in memory and especially verbal learning skills after COVID-19, strengthened the widespread view in the literature.
It has been noted that there are different results regarding the effects of COVID-19 on attention skills in the literature. Hampshire et al. [27] found that the digit span test was not effective in hospitalized COVID-19 patients receiving respiratory support, but was significantly effective in patients who did not need respiratory support although they had respiratory symptoms in the hospital or at home, and had no respiratory symptoms. Hosp et al. [28] also observed deterioration in the digits backward in most of the COVID-19 patients showing cognitive impairment symptoms according to MoCA. Zhou et al. [34] showed that there was a deterioration in continuous attention skill, although they did not find a significant difference in the digit span test, and that there was a relationship between the C-reactive protein level and the reaction time in the attention test. In a systematic study compiled from studies whose participants had a mean age of over 60, with the exception of one, it was stated that the increase in TNFα and IL-1β, which impair neural firing, might affect attention, although no definite conclusions could be reached [35]. In our study on the patients who did not receive respiratory support, we did not find a significant difference in the digits forward, which measures span of attention, short-term and working memory between the patients with COVID-19 and the healthy control group. Considering other studies in the literature, it is understood that it is difficult to reach a consensus about the effects of COVID-19 on attention skills since the participants consisted of the elderly population and factors such as the types of attention evaluated, the severity of the disease, the presence of oxygen demand, and the level of infection differ [26, 27, 30, 34].
It was observed in previous studies that executive functions were evaluated as a subsection of a screening test or with one or more detailed tests [26, 34]. Despite the differences in methodology, it was mentioned in most studies that executive functions were most impacted after COVID-19 [4, 31, 36]. On the other hand, Zhou et al. found no difference in the executive functions evaluated using the TMT in the COVID-19 group compared to the control group [34]. In our study, we also found significant differences in phonemic fluency and TMT-A results in the experimental group compared to the healthy control group. It has been reported in the literature that cognitive deficits that occur after infection could be affected by many factors. Almeria et al. [26] suggested that oxygen demand is associated with deficits in executive functions, while Alemanno et al. [2] stated that age is associated with cognitive disorders. It is also one of the points underlined that the heterogeneity in the study methodologies makes it difficult to make a final decision [37].
While the impact of COVID-19 on memory, attention, and executive functions has been extensively studied, studies on visual perception appear to be limited. Hampshire et al. [27] found that the visual attention performance of COVID-19 patients was significantly affected. Zhou et al. [34], however, did not find any significant differences in the results of tests evaluating visual perception and visual memory performance. Our study concluded that visual perceptual functions measured using the ROCF test were significantly affected. The low copying performance shows that the planning ability is also affected. In addition, the significant deterioration observed in the Clock-Drawing Test results supports this. Our results clearly show that visual structuring skills, visual attention, and memory are affected in people suffering from COVID-19. However, more studies evaluating visual perceptual skills are needed in the literature.
As a result of studies on the neuropsychiatric condition in COVID-19, post-traumatic stress disorder [36, 38], depression [2, 39, 40], anxiety, obsessive–compulsive symptoms, and insomnia [40] symptoms were observed in people following the disease [41]. Our study found that the NPI scores questioning behavioral symptoms such as depression, anxiety, and apathy in the individuals with COVID-19 were highly significantly affected compared to the healthy control group, and especially apathy, sleep and night-time behaviors, and appetite and eating changes made a significant difference. We believe that the reason why depression and anxiety did not make a significant difference in the healthy control group is related to the fact that the pandemic process causes stress, depression, and anxiety [42] in the general population.
As stated in most of the published studies in the literature, the association between cognitive impairment and disease-related variables such as disease severity has been researched [43,44,45]. However, no consensus has been reached. Manera et al. [43] stated that mild-to-moderate patients requiring assistive ventilation who however did not admit to an ICU were more likely to suffer from cognitive deficits. As mentioned in another study, a mild or moderate COVID-19 infection may be associated with cognitive impairments [44]. In addition, Mattioli et al. [45] stated that there is not any cognitive impairment in mild and moderate symptoms of COVID-19 patients who did not require any oxygen support. With this study, we analyzed whether there is a relationship between disease severity and cognitive impairment in the study group which consisted of the individuals with COVID-19 infection that did not require any respiratory support and oxygen support. There was no significant relationship between cognitive skills and disease severity parallel to the results of the Mattioli et al. study.
We reviewed the literature and found that the studies evaluating the effect of COVID-19 on cognitive functions were insufficient to make a judgment, and no study conducted with the young population was found. Our study differs from the others in that the sample group was young, all patients had the disease process at home, there were no patients with severe disease, and no one received respiratory support. We believe that our research will shed light on the literature by establishing its original value with all these aspects.
Limitations
The limitation of our study is that the cognitive and psychological state of the participants in the experimental group before they picked up the disease was not known. Besides, due to time constraints, the participants could not be subjected to a method requiring more sample groups, or a classification according to whether they received medical treatment or to the types of antiviral treatment they received. However, we believe that it would be better to make this distinction to distinguish the effects of medical treatment on cognitive functions.
Conclusion
It is stated that COVID-19 can affect CNS and the cognitive skills of individuals. Studies on the elderly population have shifted the focus to this segment because of greater effects. The results of our study demonstrate that the cognitive skills of young individuals with mild to moderate COVID-19 infection may be affected in the acute phase, independent of disease severity, pointing to the lack of data on this subject. The long-term consequences of the cognitive effects of COVID-19 that we observe in the acute phase should be investigated with randomized, more comprehensive, and well-designed studies.
References
Miners S, Kehoe PG, Love S (2020) Cognitive impact of COVID-19: looking beyond the short term. Alzheimer’s Res Ther 12(1):170. https://doi.org/10.1186/s13195-020-00744-w
Alemanno F, Houdayer E, Parma A, Spina A, Del Forno A, Scatolini A, Angelone S, Brugliera L, Tettamanti A, Beretta L, Iannaccone S (2021) COVID-19 cognitive deficits after respiratory assistance in the subacute phase: a COVID-rehabilitation unit experience. PLoS One 16. https://doi.org/10.1371/journal.pone.0246590
Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, Chang J, Hong C, Zhou Y, Wang D, Miao X, Li Y, Hu B (2020) Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol 77:683–690. https://doi.org/10.1001/jamaneurol.2020.1127
Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, Collange O, Boulay C, Fafi-Kremer S, Ohana M, Anheim M, Meziani F (2020) Neurologic features in severe SARS-CoV-2 infection. N Engl J Med 382(23):2268–2270. https://doi.org/10.1056/NEJMc2008597
Varatharaj A, Thomas N, Ellul MA, Davies NWS, Pollak TA, Tenorio EL, Sultan M, Easton A, Breen G, Zandi M, Coles JP, Manji H, Al-Shahi Salman R, Menon DK, Nicholson TR, Benjamin LA, Carson A, Smith C, Turner MR, Solomon T, Kneen R, Pett SL, Galea I, Thomas RH, Michael BD, CoroNerve Study Group (2020) Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. Lancet Psychiatry 7(10):875–882. https://doi.org/10.1016/S2215-0366(20)30287-X
Baker HA, Safavynia SA, Evered LA (2021) The ‘third wave’: impending cognitive and functional decline in COVID-19 survivors. Br J Anaesth 126(1):44–47. https://doi.org/10.1016/j.bja.2020.09.045
Bandala C, Cortes-Altamirano JL, Reyes-Long S, Lara-Padilla E, Ilizaliturri-Flores I, Alfaro-Rodríguez A (2021) Putative mechanism of neurological damage in COVID-19 infection. Acta Neurobiol Exp 81(1):69–79. https://doi.org/10.21307/ane-2021-008
Maugeri G, Musumeci G (2021) Adapted physical activity to ensure the physical and psychological well-being of COVID-19 patients. J Funct Morphol Kinesiol 6(1):13. https://doi.org/10.3390/jfmk6010013
Solianik R, Mickevičienė D, Žlibinaitė L, Čekanauskaitė A (2021) Tai chi improves psychoemotional state, cognition, and motor learning in older adults during the COVID-19 pandemic. Exp Gerontol 150:111363. https://doi.org/10.1016/j.exger.2021.111363
Killgore WDS, Cloonan SA, Taylor EC, Dailey NS (2020) Loneliness: a signature mental health concern in the era of COVID-19. Psychiatry Res 290:113117. https://doi.org/10.1016/j.psychres.2020.113117
Stewart CC, Yu L, Glover CM, Mottola G, Bennett DA, Wilson RS, Boyle PA (2020) Loneliness interacts with cognition in relation to healthcare and financial decision making among community-dwelling older adults. Gerontologist 60(8):1476–1484. https://doi.org/10.1093/geront/gnaa078
Woo MS, Malsy J, Pöttgen J, Seddiq Zai S, Ufer F, Hadjilaou A, Schmiedel S, Addo MM, Gerloff C, Heesen C, Schulze Zur Wiesch J, Friese MA (2020) Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Commun 2:1–9. https://doi.org/10.1093/braincomms/fcaa205
World Health Organization (2020) Clinical management of COVID-19, ınterim guidance. WHO reference number: WHO/2019-nCoV/clinical/2020.5 https://apps.who.int/iris/handle/10665/332196
Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53(4):695–699. https://doi.org/10.1111/j.1532-5415.2005.53221.x
Agrell B, Dehlin O (1998) The clock-drawing test. Age Ageing 27:399–403. https://doi.org/10.1093/ageing/afs149
Öktem Ö (1992) Sözel bellek süreçleri testi (SBST): Bir ön çalışma. Nöropsikiyatri Arşivi 29:196–206
Welchsler D (1987) Wechsler Memory Scale-Revised Manual. The Psychological Corporation, San Antonio, TX
Ardila A, Ostrosky-Solís F, Bernal B (2007) Cognitive testing toward the future: the example of Semantic Verbal Fluency (ANIMALS). Int J Psychol 41:324–332. https://doi.org/10.1080/00207590500345542
Stroop JR (1935) Studies of interference in serial verbal reactions. Journal of Experimental Psychology. J Exp Psychol 18:643–662. https://doi.org/10.1037/h0054651
Army Individual Test Battery. Manual of Directions and Scoring (1944) Washington: War Department, Adjutant General’s Office. https://scholar.google.com/scholar_lookup?title=Manual%20of%20Directions%20and%20Scoring&publication_year=1944&author=Army%20Individual%20Test%20Battery
Rey A (1941) L’examen psychologique dans les cas d’encéphalopathie traumatique. The psychological examination in cases of traumatic encepholopathy. Arch de Psychol 28:215–285
Meyers J, Meyers K (1995) Rey Complex Figure Test and Recognition Trial (RCFT). Psychological Assessment Resources, Odessa
Cummings JL (1997) The Neuropsychiatric Inventory: assessing psychopathology in dementia patients. Neurology 48:S10–S16. https://doi.org/10.1212/WNL.48.5_Suppl_6.10S
Sullivian GM, Feinn R (2012) Using effect size–or why the P value is not enough. J Grad Med Educ 4(3):279–282. https://doi.org/10.4300/JGME-D-12-00156.1
Warren-Gash C, Forbes HJ, Williamson E, Breuer J, Haywar AC, Mavrodaris A, Ridha BH, Rossor MN, Thomas SL, Smeeth L (2019) Human herpesvirus infections and dementia or mild cognitive impairment: a systematic review and meta-analysis. Sci Rep 9:1–10. https://doi.org/10.1038/s41598-019-41218-w
Almeria M, Cejudo JC, Sotoca J, Deus J, Krupinski J (2020) Cognitive profile following COVID-19 infection: clinical predictors leading to neuropsychological impairment. Brain, Behav, Immun - Health 9:100163. https://doi.org/10.1016/j.bbih.2020.100163
Hampshire A, Trender W, Chamberlain SR, Jolly AE, Grant JE, Patrick F, Mazibuko N, Williams SC, Barnby JM, Hellyer P, Mehta MA (2020) Cognitive deficits in people who have recovered from COVID-19 relative to controls: an N=84,285 online study. medRxiv 39:101044. https://doi.org/10.1016/j.eclinm.2021.101044
Del Brutto OH, Wu S, Mera RM, Costa AF, Recalde BY, Issa NP (2021) Cognitive decline among individuals with history of mild symptomatic SARS-CoV-2 infection: a longitudinal prospective study nested to a population cohort. Eur Acad Neurol 28(10):3245–3253. https://doi.org/10.1111/ene.14775
Patel R, Savrides I, Cahalan C, Doulatani G, O’Dell MW, Toglia J, Jaywant A (2021) Cognitive impairment and functional change in COVID-19 patients undergoing inpatient rehabilitation. medRxiv 44(3):285–288. https://doi.org/10.1097/MRR.0000000000000483
Hosp JA, Dressing A, Blazhenets G, Bormann T, Rau A, Schwabenland M, Thurow J, Wagner D, Waller C, Niesen WD, Frings L, Urbach H, Prinz M, Weiller C, Schroeter N, Meyer PT (2021) Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19. Brain 144(4):1263–1276. https://doi.org/10.1093/brain/awab009
Miskowiak KW, Johnsen S, Sattler SM, Nielsen S, Kunalan K, Rungby J, Lapperre T, Porsberg CM (2021) Cognitive impairments four months after COVID-19 hospital discharge: pattern, severity and association with illness variables. Eur Neuropsychopharmacol 46:39–48. https://doi.org/10.1016/j.euroneuro.2021.03.019
Prieto GA, Tong L, Smith ED, Cotman CW (2019) TNFα and IL-1β but not IL-18 suppresses hippocampal long-term potentiation directly at the synapse. Neurochem Res 44(1):49–60. https://doi.org/10.1007/s11064-018-2517-8
Ritchie K, Chan D, Watermeyer T (2020) The cognitive consequences of the COVID-19 epidemic: collateral damage? Brain Commun 2:1–5. https://doi.org/10.1093/braincomms/fcaa069
Zhou H, Lu S, Chen J, Wei N, Wang D, Lyu H, Shi C, Hu S (2020) The landscape of cognitive function in recovered COVID-19 patients. J Psychiatr Res 129:98–102. https://doi.org/10.1016/j.jpsychires.2020.06.022
Tancredi V, D’Arcangelo G, Grassi F, Tarroni P, Palmieri G, Santoni A, Eusebi F (1992) Tumor necrosis factor alters synaptic transmission in rat hippocampal slices. Neurosci Lett 146(2):176–178. https://doi.org/10.1016/0304-3940(92)90071-e
Ardila A, Lahiri D (2020) Executive dysfunction in COVID-19 patients. Diabetes Metab Syndr 14(5):1377–1378. https://doi.org/10.1016/j.dsx.2020.07.032
Daroische R, Hemminghyth MS, Eilertsen TH, Breitve MH, Chwiszczuk LJ (2021) Cognitive impairment after COVID-19—a review on objective test data. Front Neurol 12:699582. https://doi.org/10.3389/fneur.2021.699582
Bo HX, Li W, Yang Y, Wang Y, Zhang Q, Cheung T, Wu X, Xiang YT (2020) Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol Med 51(6):1052–1053. https://doi.org/10.1017/S0033291720000999
Zhang J, Lu H, Zeng H, Zhang S, Du Q, Jiang T, Du B (2020) The differential psychological distress of populations affected by the COVID-19 pandemic. Brain Behav Immun 87:49–50. https://doi.org/10.1016/j.bbi.2020.04.031
Pistarini C, Fiabane E, Houdayer E, Vassallo C, Manera MR, Alemanno F (2021) Cognitive and emotional disturbances due to COVID-19: an exploratory study in the rehabilitation setting. Front Neurol 12:643646. https://doi.org/10.3389/fneur.2021.643646
Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, Melloni EMT, Furlan R, Ciceri F, Rovere-Querini P, COVID-19 BioB Outpatient Clinic Study group, Benedetti F (2020) Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain, Behav Immun 89:594–600. https://doi.org/10.1016/j.bbi.2020.07.037
Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, Rasoulpoor S, Khaledi-Paveh B (2020) Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health 16(1):57. https://doi.org/10.1186/s12992-020-00589-w
Manera MR, Fiabane E, Pain D, Aiello EN, Radici A, Ottonello M, Padovani M, Wilson BA, Fish J, Pistarini C (2022) Correction to: Clinical features and cognitive sequelae in COVID-19: a retrospective study on N=152 patients. Neurol Sci 43(1):753. https://doi.org/10.1007/s10072-021-05766-2
Henneghan AM, Kimberly AL, Gill E, Kesler SR (2022) Cognitive impairment in non-critical, mild-to-moderate COVID-19 survivors. Front Psychol 13:770459. https://doi.org/10.3389/fpsyg.2022.770459
Mattioli F, Stampatori C, Righetti F, Sala E, Tomasi C, De Palma G (2021) Neurological and cognitive sequelae of Covid-19: a four month follow-up. J Neurol 268(12):4422–4428. https://doi.org/10.1007/s00415-021-10579-6
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Informed consent
Consent to participate all the patients have given their written informed consent.
Ethical approval
The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. The study was approved by the Non-Interventional. Interventional Clinical Research Ethics Committee with the decision number E-10840098-772.02-65171 on December 10, 2020, and was registered on ClinicalTrials.gov (NCT04978246).
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Akıncı, B., Oğul, Ö.E., Hanoğlu, L. et al. Evaluation of cognitive functions in adult individuals with COVID-19. Neurol Sci 44, 793–802 (2023). https://doi.org/10.1007/s10072-022-06562-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-022-06562-2