
Key Points
-
Human papillomaviruses (HPVs) are the aetiological agents of approximately 5% of human cancers, most notably those of the cervix, oropharynx, anus, vulva, vagina and penis.
-
In clinical efficacy trials, vaccines based on virus-like particles (VLPs) were highly effective as prophylactic vaccines, preventing infection and the hyperproliferative lesions that are caused at the cervix, anus, vulva, vagina and penis by the HPV types targeted by the vaccines.
-
Two HPV VLP-containing vaccines, Gardasil and Cervarix, are licensed in many countries for general distribution to adolescent girls and young women and, in some countries, to adolescent boys and young men.
-
The high-titre, durable antibody responses that are induced by the VLPs are believed to be the primary mediators of protection.
-
Unique aspects of the viral infectious process, including initial binding to the epithelial basement membrane and slow cell entry kinetics, might account for the exceptional susceptibility of HPV to inhibition by vaccine-induced antibodies.
-
The insights learned from the remarkable efficiency of prophylactic HPV vaccines could potentially be applied to the design of effective vaccines for preventing the spread of other sexually transmitted viruses, such as HIV and HSV. However, differences in basic virological characteristics might make it difficult to directly transfer this knowledge between viruses.
Abstract
An estimated 5% of human cancers are caused by human papillomavirus (HPV) infections, and most of these cancers are of the cervix. Two prophylactic HPV vaccines that target the two most oncogenic virus types, HPV16 and HPV18, are now commercially available. In controlled clinical trials, the vaccines proved to be effective at preventing incident anogenital infection and the associated neoplastic disease that is induced by these virus types. Here, we highlight the specific aspects of HPV biology and vaccine composition that are likely to contribute to the efficacy of these vaccines, and we discuss how these particular features might or might not be relevant for the development of effective vaccines against other sexually transmitted viruses such as HIV and herpes simplex virus (HSV).
Similar content being viewed by others

Main
The development of antimicrobial vaccines is undoubtedly one of the greatest triumphs of biomedical research. Along with antibiotics and clean water, vaccines have made a substantial contribution to the dramatic reduction in human suffering and death caused by infectious agents over the past two centuries1. Given the extraordinary effectiveness of vaccines against a wide array of bacterial and viral pathogens, the failure to develop successful vaccines against the most common sexually transmitted pathogens, especially HIV, has been both surprising and frustrating. The only notable exception is the development of prophylactic vaccines against genital human papillomaviruses (HPVs). In recently concluded clinical trials, these vaccines were found to be extremely effective at preventing sexually transmitted infection and the neoplastic diseases that are induced by the targeted HPV types2,3,4,5,6,7. The vaccines are now licensed in many countries worldwide for the prevention of cervical and other HPV-associated cancers as well as various additional hyperproliferative diseases. It is therefore interesting to assess why the HPV vaccines have succeeded, whereas those targeting other sexually transmitted infections (STIs) have failed. Are there lessons to be learned from the HPV vaccines that might inform successful development of vaccines against other STIs? In this Review, we briefly discuss the association of HPVs with human cancer and other neoplastic diseases, describe the composition of the two commercial vaccines, and summarize their efficacy in clinical trials and their emerging effectiveness in general vaccination programmes. We then discuss the factors that are likely to contribute to the remarkable success of these vaccines and comment on how the lessons that we have learned from the HPV vaccines might influence the future of vaccine development for other STIs.
HPV and cancer
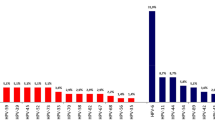
Papillomaviruses are small non-enveloped viruses with circular double-stranded DNA genomes, and they infect the stratified squamous epithelium of a wide array of mammals and other vertebrates8. Most of the >100 known HPV genotypes induce either asymptomatic epithelial infection or benign epithelial hyperplasia. However, persistent infection by any of about 15 'high-risk' mucosatropic virus types is associated with progression to carcinoma of the cervix, vulva, vagina, penis, anus and oropharynx9. The sexually transmitted HPV infections that lead to these cancers are common, but they rarely progress to cancer. Nevertheless, it has been estimated that approximately 5% of all human cancers are caused by HPV infection, mostly with HPV16 or HPV18 (Ref. 10). The worldwide incidence of these cancers and the fraction attributed to HPV infections vary widely (Fig. 1a). Vaccine developers have primarily targeted cervical cancer, because it constitutes the majority of HPV-associated cancer cases worldwide10,11. However, 85% of cervical cancer cases occur in women living in underdeveloped countries, in large measure because they do not have access to effective cervical cancer screening programmes. Because screening programmes can reduce cervical cancer rates by more than 80%12, other HPV-associated cancers constitute a greater proportion of the HPV-attributed cancer burden in most developed countries, and a greater fraction of the cancers in these countries occur in men13 (Fig. 1b). Phylogenetically distinct 'low-risk' virus types, particularly HPV6 and HPV11, are the most common aetiological agents of sexually transmitted genital warts (condyloma acuminata)14, and other low-risk virus types frequently cause common hand and foot warts in both children and adults15.

The breakthrough in establishing the causal relationship between HPV infection and cervical cancer came in 1983, when Harald zur Hausen and colleagues reported the cloning of HPV16 from a cervical carcinoma and the detection of this virus type in about 50% of a case series of cervical cancers16. The isolation of other high-risk virus types, including HPV18, HPV31, HPV33, HPV35, HPV45, HPV52 and HPV58, soon followed. Laboratory-based studies in the 1980s led to the characterization of the immortalizing and transforming properties of the HPV oncoproteins E6 and E7; this was followed by the discovery of their biochemical activities in inhibiting the tumour suppressor genes P53 (also known as TP53) and RB (also known as RB1; encoding retinoblastoma-associated protein), respectively, and the detection of their continued expression in cervical carcinomas17. Case control epidemiology studies in the early to mid 1990s established the presence of high-risk HPV genomes in virtually all cervical cancers, with HPV16 or HPV18 detected in approximately 70% of cases worldwide18. Subsequent prospective studies in the mid to late 1990s strongly supported a causal relationship by establishing that high-risk HPV infection is maintained during all stages of carcinogenic progression, from benign productive infection to cervical intraepithelial neoplasia grade III (CIN III), the accepted precursor lesion for cervical cancer19. The proposal in 1999 that HPV infection be considered the necessary cause of cervical cancer coincided with the initiation of clinical efficacy trials of HPV vaccines, reflecting the strong public-health rationale for their further academic and commercial development20.
HPV vaccines
The antigens in the two commercial HPV vaccines are virus-like particles (VLPs) composed of L1, the major capsid protein of HPV (Box 1). Assembly of L1 into VLPs was first reported for bovine papillomavirus type 1 (BPV-1) in 1992, and reports of HPV L1 assembly into VLPs soon followed21,22,23. Cervarix, manufactured by GlaxoSmithKline Biologicals, contains the L1 VLPs of HPV16 and HPV18 and is manufactured in insect cells infected with recombinant baculovirus. Gardasil, manufactured by Merck and produced in yeast, contains VLPs of HPV6, HPV11, HPV16 and HPV18, and therefore targets HPVs associated with both cancer and genital warts (Table 1). Both vaccines contain an aluminium salt adjuvant that precipitates the VLPs. This ensures a slow release of the antigen and the activation of invading monocytes after injection, leading to heightened B cell responses. In addition, Cervarix contains monophosphoryl lipid A (MPL; a detoxified form of lipopolysaccharide), which activates the innate immune response through Toll-like receptor 4 (TLR4), leading to increased antibody responses to the VLPs24. Cervarix is the first prophylactic vaccine containing a TLR agonist that has been approved by the US FDA. Both vaccines are administered by intramuscular injection in three doses over 6 months, although the recommended timing of the second dose varies between the two vaccines (Table 1).
Efficacy and effectiveness studies
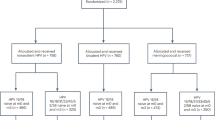
Randomized clinical trials sponsored by GlaxoSmithKline Biologicals, Merck and the US National Cancer Institute established the remarkable efficacy of the vaccines (Table 2). End-of-study analyses of 4-year trials for both vaccines reported a 100% efficacy in preventing HPV16- and HPV18-associated CIN III dysplasia in young women who had no evidence of genital HPV infection at enrolment and who received at least one dose of the vaccine5,6. There was also strong protection against lower grades of cervical dysplasia caused by the vaccine-targeted HPV types. Most vaccinated women never tested positive for genital HPV DNA of these types using sensitive PCR-based detection methods, implying that the vaccines generally confer sterilizing immunity. Most breakthrough infections occurred in the first year of the trials, suggesting that they were mostly due to the emergence of pre-existing infections3,25. Furthermore, there was no evidence for waning of protection, at least not for the first 8.4 years after vaccination26. Surprisingly, 4 years after vaccination, protection from persistent HPV16 and HPV18 infections was as high in women vaccinated with a single dose of Cervarix as in women vaccinated with two or three doses27. However, additional studies will be needed to determine whether fewer than three doses will provide comparable long-term protection to that provided by the recommended protocol. Cervarix was also shown to protect young women from anal HPV16 or HPV18 infections28. In young women, Gardasil also conferred >95% protection against genital warts, and against vulvar and vaginal dysplasias associated with the HPV types targeted by the vaccine6. Furthermore, Gardasil was recently shown to be highly effective at preventing anal infection, genital warts and anal intraepithelial neoplasia (AIN) in young men who had no evidence of infection with the targeted virus types at enrolment2,7 (Table 2). Unfortunately, protection from infection and neoplastic disease is virus type restricted, with partial cross-protection detected against only specific virus types that are closely related to HPV16 or HPV18 (Refs 29, 30). In addition, there is no evidence that either vaccine acts therapeutically to induce clearance of existing infections or prevent their progression to high-grade dysplasia31,32. However, there is some evidence that the vaccines reduce the risk of recurrences following treatment of anogenital lesions33.
The results of the Phase III clinical trials outlined above have led to worldwide licensure of both vaccines for older girls and young women, and more recently of Gardasil for older boys and young men. Crucial issues that were raised during the implementation of the vaccination programmes are outlined in Box 2. Evidence for the effectiveness of these vaccines now that they are in general use has begun to emerge in those countries that adopted high-coverage vaccination programmes for females early after licensure. In sentinel surveillance studies in Australia, the incidence of genital warts decreased by 59% in women younger than 27 years old, and the incidence of CIN III dysplasias decreased by 48% in women younger than 18 years old34,35. By contrast, a decrease in infection rates was not observed in older women who were not targeted for vaccination. Interestingly, the incidence of genital warts in young heterosexual men (who were also not targeted for vaccination) dropped by 39%, suggesting the rapid establishment of substantial herd immunity, although there was no decrease in incidence among men who have sex with men.
Effector mechanisms
Key role of antibodies in mediating protection. Several lines of evidence point to vaccine-induced antibodies as being the primary, if not the sole, mediators of the protection induced by the prophylactic HPV vaccines. First, the L1 VLPs induce high titres of virion-neutralizing serum antibodies in vaccinated individuals after intramuscular injection. This strong immunogenicity was first demonstrated by in vitro neutralization assays using sera from rabbits vaccinated with either BPV VLPs or authentic BPV virions22, and was subsequently confirmed for HPV VLPs using the sera from vaccinated animals and, eventually, people36,37. These neutralization assays primarily used cell-derived pseudovirions with an encapsidated marker gene-expressing plasmid38 (Box 1). The second line of evidence for the role of antibodies in HPV vaccine-mediated immunity comes from the finding that passive transfer of immune sera from VLP-vaccinated animals to naive animals protects the naive animals from experimental challenge with the corresponding animal papillomavirus in canine and rabbit models39,40. To extend this observation to vaccine-targeted HPVs, a mouse cervicovaginal-challenge model was developed in which infection with HPV pseudovirions is monitored by light emission as a result of luciferase expression from the encapsidated plasmid41 (Fig. 2). Remarkably, passively transferred sera from VLP-vaccinated mice protect against experimental cervicovaginal infection when the transferred sera are diluted up to 10,000-fold in the circulation of the recipient animals42. These antibody levels are more than 100-fold lower than the minimum levels detectable in the sera of the recipient mice using a pseudovirus-based in vitro neutralization assay. Taken together, these results established that VLP-induced antibodies are sufficient to induce potent protection against tissue infection by papillomaviruses, including high-dose infection of the female genital tract by oncogenic HPVs. The third line of evidence implicating antibodies in HPV vaccine-induced immunity is the fact that in the clinical trials there was a spectrum of partial protection against virus types not included in the vaccines, and these virus types largely mirror the HPV types for which in vitro neutralizing titres could be detected43. Notably, the titres against heterologous virus types, when detected, are more than 100-fold lower than the titres against the HPV types included in the vaccines.

Serum is withdrawn from a mouse that has been vaccinated with human papillomavirus (HPV) virus-like particles (VLPs); the serum is diluted (step 1) and transferred by intraperitoneal injection into a naive mouse70 (step 2). After 24 hours, serum from the recipient mouse is withdrawn, and the in vitro neutralization titre of this serum (determined by neutralization of pseudovirus infectivity) is measured (step 3). The recipient mouse is then challenged by intravaginal instillation of luciferase-expressing HPV pseudovirions (step 4). After 2 days, the extent of infection is assessed by intravaginal instillation of the luciferase substrate, luciferin (step 5). The luciferase catalyses an ATP-dependent reaction that results in the emission of light by luciferin. By measuring the amount of light emitted, the degree of infection with HPV pseudovirions can be estimated for the recipient 'immune' mouse. As a comparison, the same procedure is carried out using serum withdrawn from a mouse before vaccination with VLPs; the recipient mouse in this case is referred to here as 'pre-immune'.
It is unlikely that CD4+ T cell effector functions are involved in protection because the vaccines induce different responses owing to the use of different adjuvants: Cervarix induces a T helper 1 (TH1) cell-dominated response, whereas Gardasil induces a TH2 cell-dominated response, but both vaccines are highly protective44,45. Potent CD8+ T cell responses against L1 are generated after VLP vaccination; however, unique aspects of the papillomavirus life cycle make it unlikely that these T cells are involved in protection46. Specifically, L1 is not detectable in the lower layers of the stratified squamous epithelium47, as its expression is restricted to the terminally differentiated keratinocytes in the upper layers (where the gene encoding L1 is activated in response to differentiation-specific signals generated by the host cell). It is therefore unlikely that the CD8+ T cell responses, which are directed against these L1-containing terminally differentiated keratinocytes, would eliminate the infected basal cells in which the infection is maintained, given that they are separated by several layers of intervening cells.
On the basis of antibody immunobridging studies, national regulatory agencies such as the US FDA have tacitly acknowledged that antibodies are likely to be the main effectors of protection (or at least a surrogate marker for protection), in that these agencies have extended vaccine licensure to groups for which there are no efficacy data from clinical trials. Most importantly, the finding that girls and boys aged 10–15 years generate a stronger antibody response to the vaccines than 16–25-year-olds has resulted in public-sector vaccination campaigns that principally focus on the younger age group48,49,50.
Transfer of antibodies to the infected site. If antibodies are the essential effectors for HPV vaccines, the question arises as to how VLP vaccine-induced antibodies reach the site of HPV infection in the mucosal epithelium, especially the female genital tract. Intramuscular injection of VLPs (and other antigens) primarily induces a serum immunoglobulin G (IgG) response with little, if any, secretory IgA (sIgA)51. Fortunately, systemically induced IgG can reach the sites of genital mucosal infection by two mechanisms. First, unlike for other mucous secretions, there is substantial transudation of systemic IgG into cervicovaginal mucus, most likely via interactions with neonatal Fc receptor52. In an early clinical immunogenicity study, the VLP-specific IgG titres in vaccinated women were approximately tenfold higher in the cervicovaginal mucus than in the serum. However, VLP-specific IgG, and IgG in general, drop by tenfold in response to changing sex hormone levels at the time of ovulation53. The second mechanism is direct exudation of systemic antibodies at the site of infection. Studies in the mouse cervicovaginal model revealed that infection of keratinocytes requires HPV capsids to initially bind to the epithelial basement membrane at sites where the overlying epithelium is permeabilized or traumatized41 (Fig. 3). Thus, the virions are exposed to an increasing gradient of exuded antibodies as they make their way to the initial site of infection. The exudation mechanism might completely account for antibody-mediated protection, as the clinical trials reported excellent protection from genital warts, which arise on cornified skin (sites where protection by transuded antibodies is unlikely to occur)6.

a | Human papillomavirus (HPV) virions cannot bind or infect intact squamous epithelium. They must first bind the basement membrane via heparan sulphate proteoglycans. Then, in a process that takes several hours, they must undergo a series of conformational changes, beginning with furin-mediated cleavage of the minor capsid protein, L2 (yellow), to expose their receptor-binding site on the major capsid protein, L1 (blue), followed by binding to the cell surface receptor and infection of basal epithelial keratinocytes. b | High levels of virus-like particle (VLP)-induced antibodies prevent attachment of the virus to the basement membrane, and this in turn prevents the conformational changes required for cell surface binding. Virus–antibody complexes associate with neutrophils in the cervicovaginal mucus. c | Low levels of VLP-induced antibodies permit basement membrane attachment and the conformational changes leading to furin-mediated L2 cleavage, but they prevent a stable association of the virion with the cell surface. N, amino.
Why do the vaccines work so well?
If antibodies are the primary effectors of protection for VLP-based HPV vaccines, this question can essentially be rephrased as “Why are the VLP vaccines so effective at inducing strong antibody responses, and why are the antibodies that they induce so effective at preventing infection in vivo?” In the following section, the case is made that multiple factors contribute to the effectiveness of the vaccines, including characteristics of the immunogen and specific aspects of the viral infectious process.
Intrinsic immunogenicity of VLPs. VLPs retain the ordered, repetitive and closely arrayed arrangement of epitopes that is found on the surface of native viruses54 (Box 1), as well as on the surfaces of other microbial structures such as bacterial pili. Almost two decades ago, Bachman and Zinkernagel proposed that this arrangement of epitopes, with a characteristic 50–100 Å spacing, is specifically recognized as foreign by B cells, as elements with this spacing are not found on surfaces of the mammalian body that are routinely exposed to the systemic immune system55. Many studies have subsequently confirmed that multivalent engagement of B cell receptors by repetitive epitopes on natural microbial or synthetic immunogens generates an exceptionally strong activation of, and survival signal in, B cells56. A virus-like display of central self-antigens, for instance on the surface of HPV VLPs, can even break peripheral B cell tolerance to self, with display in closely spaced arrays being the key determinant57. Therefore, it is not surprising that the clinical trials revealed strong and consistent antibody responses to the VLPs, with almost 100% seroconversion even when the VLPs were administered without an adjuvant58,59.
The antibody response to VLP vaccination is also durable. It generally drops approximately tenfold over the first 1.5 years and then stabilizes at a plateau level that remains constant for as long as vaccinated individuals have been examined (up to 8.4 years in some studies)26,37. The continued expression of constant antibody levels over many years is probably due to long-lived plasma cells residing in the bone marrow60. This pattern is similar to that observed for live attenuated virus vaccines, with which stable antibody responses to viral structural elements are detectable for decades after vaccination61. The fact that essentially no breakthrough infections were observed in the later years of the clinical trials, well after the antibody titres had plateaued, suggests that the HPV vaccines will confer substantially longer-term protection3,25,26.
Several other factors also contribute to the high immunogenicity of papillomavirus VLPs. First, they are 55–60 nm spheres, an optimal size and shape for direct trafficking to lymph nodes after parenteral delivery; presumably, these VLPs are then efficiently presented to B cells by follicular dendritic cells (DCs) in the lymph nodes56. Second, the VLPs bind directly to several types of human immunocytes, including monocytes, macrophages, and myeloid and plasmacytoid DCs. These interactions induce various innate immune responses, including the production of pro-inflammatory cytokines (such as interleukin-1β (IL-1β), IL-6, IL-8, IL-12, interferon-α (IFNα), IFNγ and tumour necrosis factor (TNF)), and lead to the acute phenotypic and functional maturation of DCs, thereby promoting adaptive immune responses62,63. Third, particulate antigens such as VLPs are especially effective in the induction of major histocompatibility complex (MHC) class II-restricted responses in CD4+ TH cells, and these responses aid in the induction of B cell responses.
Characteristics of L1 neutralization epitopes. Essentially, all L1 epitopes that are recognized by neutralizing antibodies are conformation dependent. These epitopes are retained by VLPs but lost in denatured L1 or in L1 peptides, thus explaining the unsuccessful attempts to develop prophylactic vaccines against papillomaviruses before the generation of VLPs22,64. However, detailed studies have established that the human polyclonal response to VLP vaccination induces neutralizing antibodies that recognize multiple distinct L1 epitopes65. The breadth of the neutralizing response to the VLPs probably explains why the antibodies generated against one variant of HPV16, for instance, are able to neutralize other HPV16 variants with L1 sequences that differ from the targeted sequence by a small number of amino acids66. Therefore, although distinct viral genotypes essentially represent distinct serotypes, it is unlikely that functionally distinct serotypes exist within a given genotype. Consistent with this conjecture, in the Phase III efficacy trials the VLP vaccines demonstrated a similar high efficacy in many sites across the globe, despite the fact that different variants of the HPV types might predominate locally67. Given the breadth of the neutralizing antibody response to the VLPs, it is unlikely that a viable escape mutant could develop via a single amino acid change in L1. The likelihood of the rapid development of viable escape mutants with multiple changes in L1 is also greatly diminished by the fact that HPVs have low mutation rates, like human genes68 (discussed below).
Mechanism of tissue infection. Recently obtained insights into the mechanism and dynamics of HPV infection of cervicovaginal epithelium in a mouse model suggest that unique aspects of the HPV infectious process may contribute as much to the high efficacy of the vaccine as the high intrinsic immunogenicity of the VLPs69. Infection of the epithelium is initiated by binding of the capsid to heparan sulphate proteoglycans (HSPGs) on the basement membrane, which are exposed at sites of trauma (Fig. 3a). Before the virion can bind to the target cell (the basal epithelial keratinocyte), it must undergo a conformational change that exposes the amino terminus of minor capsid protein L2 for cleavage by cellular furin or cellular proprotein convertase 5 (PC5; also known as PC6 and PCSK5). This cleavage is required for exposure of the keratinocyte-binding determinant, presumably located on L1. Binding of the keratinocyte-binding determinant to a currently unknown keratinocyte receptor leads to virus internalization and, ultimately, viral infection. Each step in this process is remarkably slow. For instance, after the virus binds to the basement membrane, it takes several hours for the L2 cleavage peptide to be exposed, and the capsids subsequently remain on the cell surface for several hours before internalization. The infection is not detected until at least 1 day after intravaginal application of the virus, and peak infection is delayed until day 2 or day 3 (Ref. 41). Thus, the virus is exposed for long periods at multiple steps of the infection cycle, which would facilitate interactions with the VLP-induced antibodies to prevent infection.
Antibody-mediated protection at the tissue level. Studies involving active VLP vaccination and passive transfer of immune sera containing VLP-induced antibodies have revealed two distinct mechanisms whereby VLP-induced antibodies can prevent cervicovaginal infection70. At high levels, VLP-induced antibodies prevent binding to the basement membrane, presumably by occluding the HSPG-binding sites on the virion (Fig. 3b). When antibody levels are low, the virions bind to the basement membrane and L2 proteolysis occurs; however, stable transfer of the virus particles to the cell surface at later time points appears to be perturbed (Fig. 3c). One possible explanation for this observation is that the VLP-induced antibodies occlude the keratinocyte-binding site that is exposed by L2 cleavage. A lower affinity of the virion for the cell surface receptor than for basement membrane HSPGs might explain the difference in the level of antibody needed to inhibit the two interactions. In this scenario, low antibody occupancy of the virion surface might be sufficient to prevent stable virion binding to the cell without impeding binding to the basement membrane. However, other explanations are possible. For instance, monocytes and neutrophils that are attracted to the site of trauma might efficiently scavenge the basement membrane-bound capsid–antibody complexes via interactions with the Fc receptor. In any case, the unexpected finding that in vivo protection requires substantially lower levels of antibodies than those required for in vitro neutralization certainly supports the contention that at least one mechanism of infection inhibition exists in vivo that is not detected in the in vitro neutralization assays42.
Viral strategies to circumvent protective antibodies. Some viruses have evolved mechanisms to either decrease the intrinsic immunogenicity of their virions or specifically inhibit the activity of the antibodies that they induce, but there is no evidence that HPVs have evolved any such mechanisms. However, these viruses have adopted an alternative strategy to limit their exposure to the systemic immune system. This is accomplished by restricting expression of the capsid proteins to delay assembly of the virions until the host cells have become terminally differentiated keratinocytes that are no longer under close immune surveillance. In addition, virion release occurs exclusively at the surface of the epithelium71. Hence, the induction of a detectable serum L1-specific antibody response after natural genital HPV infection is delayed by several months, if it occurs at all, and is generally low titre72. An intramuscular injection of a comparatively high dose of VLPs would be a simple and effective mechanism to bypass this immune escape mechanism.
Prospects for type replacement. The fact that HPVs and other papillomaviruses have diversified into a large number of genotypes that are also distinct serotypes strongly argues that escape from antibody-mediated neutralization has had a major role in the evolution of these viruses. However, given the slow mutation rate of the DNA genomes of these viruses, this diversification must have occurred over a long timescale. For example, rhesus papillomavirus type 1b (RhPV1), an oncogenic virus type that infects rhesus macaques, is more closely related to HPV16 than HPV18 is8. Given that there is no evidence for recombination or cross-species adaptation, it can be inferred that these two oncogenic HPVs diverged more than 20 million years ago. The slow mutation rate of the viruses, combined with the diversity of epitopes recognized by VLP-neutralizing antibodies, makes it unlikely that escape variants of the vaccine-targeted types will rapidly emerge.
It is also unlikely that existing non-vaccine-targeted types will replace vaccine-targeted types by filling a vacated ecological niche. Associations between infections by specific virus types have been observed in some cross-sectional studies; however, detailed prospective studies of cervical infections suggest that the acquisition or clearance of one type does not significantly influence the acquisition or clearance of another type73,74,75. In addition, HPV16 and HPV18 are more carcinogenic than other types, such that persistent infection by either of these types more often and more rapidly progresses to CIN III dysplasia and cancer than does infection with other HPV types76. It is unlikely that there will be direct selection for increased carcinogenesis in other virus types should HPV16 and HPV18 disappear47. Progressed lesions lack the differentiation-specific signals that are needed to produce virions, which implies that carcinogenesis is as much a dead-end for the virus as it is for the host. Therefore, although the possibility of HPV type replacement should be evaluated in populations with high rates of vaccine coverage, we doubt that it will have a major impact on the effectiveness of HPV vaccination programmes.
Lessons for STI vaccine development?
The most important lesson to be taken from the success of the HPV vaccines is the most obvious: that it is possible to develop a safe and highly effective vaccine that prevents primary genital infection by a sexually transmitted virus. The considerable scepticism toward this basic premise was well justified at the time that the HPV vaccine trials were initiated, given the many previous unsuccessful vaccine initiatives targeting other STIs. Hepatitis B virus (HBV), for which effective vaccines were produced many years ago, can be transmitted sexually. However, the effective HBV vaccines act by preventing systemic infection in the liver. The success of the HPV vaccines should encourage ongoing and future efforts to develop vaccines against other STIs. But could the development of such additional vaccines be aided by more specific lessons from the success of HPV vaccines? In the following section, this question is addressed for two viruses that cause STIs, HIV and herpes simplex virus (HSV), both of which have a long history of largely unsuccessful vaccine development efforts77,78.
Virus-like display. In our opinion, the most broadly applicable lesson is the demonstration that virus-like display of antigens can induce exceptionally strong, consistent and durable antibody responses in humans. The extensive clinical trial data support the contention that virus-like display would be an attractive strategy for safely inducing potent IgG antibody responses to other antigens in humans. There are many display platforms available, including those based on other eukaryotic viruses, bacteriophages and synthetic nanoparticles79. Interestingly, HIV might evade the induction of robust neutralizing antibody in part by displaying its major envelope protein, Env, at a low density (and in a partially non-functional form) on its surface80. Display of native trimeric Env, or of a conformationally correct subdomain from this protein, in a dense ordered array on the surface of a non-enveloped capsid, or perhaps as dense disordered arrays on liposomes81, might generate more robust antibody responses than most previous vaccine candidates. Virus-like display of HSV antigens, such as the envelope glycoproteins gB and gD, would also be expected to induce stronger antibody responses than the monomeric protein antigens that have been evaluated in clinical trials78.
Antibody responses to HIV and HSV. Although it seems quite likely that virus-like display of other viral surface antigens could induce as strong and durable an antibody response as the HPV vaccines, it may be more difficult for antibodies to prevent infections by HIV and HSV, because of differences in the basic biology of the viruses. For example, infection by HIV and HSV does not appear to have the extremely slow kinetics observed for HPV infections, so the window of opportunity for antibodies to bind the viruses before they enter the cell might be shorter. Also, trauma might be less crucial for the initiation of HIV and HSV infections than for HPV infections. Unlike HPV, HSV can infect the apical surface of intact simple columnar endocervical epithelium82, and HIV is able to translocate across an intact epithelial barrier via DCs or transcytosis through the epithelium83. If prevention of the initial infection by serum-derived HIV- and HSV-neutralizing antibodies primarily depends on transudation and not exudation (because these viruses can infect undamaged tissue sites, whereas HPV infection occurs at damaged sites, where antibodies are likely to be delivered by both exudation and transudation), then the local levels of virus-specific antibodies at the initial sites of infection might be lower and more variable for HIV- and HSV-specific antibodies than for HPV-specific antibodies.
High-titre HIV-neutralizing antibodies are not readily induced by infection with HIV or by vaccination with its major virion protein, Env, in part because of masking by a glycan shield84 that covers this immunogenic protein. By contrast, HPV L1 assembles into virions and VLPs in the nucleus, so L1 is not heavily glycosylated. Another potential obstacle is the fact that the genome of HIV is replicated via an error-prone RNA polymerase, which means that Env can rapidly evolve to escape neutralizing antibody responses in an infected individual when they arise85. Furthermore, many conserved HIV epitopes that bind broadly neutralizing antibodies, such as the viral CD4-binding domain, are not easily accessible or are only transiently exposed after cell binding86. Finally, the relevance of HIV delivery by a cell from an infected individual, the importance of cell-associated viruses for intercellular transmission within an infected person and the susceptibility of cell-associated viruses to antibody inhibition also remain uncertain83.
More optimistically, proof-of-concept studies indicate that passive transfer of HIV-neutralizing antibodies can protect against vaginal transmission of an HIV–simian immunodeficiency virus (SIV) chimeric virus87. Furthermore, HIV seems to be much less infectious than HPV, requiring 200–2,000 heterosexual exposures on average for transmission, often of a single founder virus88,89. The number of exposures needed to initiate infection is likely to be much lower for HPV, given the rapid transmission rates in newly formed couples that are discordant for HPV90. In theory, it should be easier to interrupt the spread of a poorly transmissible virus such as HIV, and the initial infection event at a mucosal site might prove to be the antibody-susceptible Achilles heel of the virus. In support of this hypothesis, the results of the recent RV 144 vaccine trial in Thailand suggest that antibodies targeting initial infection were induced in some vaccinated individuals, as the vaccine reduced acquisition rates of the infection but not the viral loads in participants who did become infected91.
The immune response that provided protection was not defined in the RV 144 trial. As was the case for HPV vaccine-induced antibodies, standard in vitro neutralization assays are unlikely to detect the full spectrum of activities conferred by HIV Env-specific antibodies that prevent an initial mucosal infection in vivo86,92. It is intriguing that HIV is less efficient than HPV at translocating through human mucus, particularly at the acidic pH that is typically found in women with a lactobacillus-dominated cervicovaginal flora93. Antibody-bound HIV is essentially stationary, even at the more neutral pH that may occur in the presence of seminal fluid. Therefore, vaccine-induced cervicovaginal antibodies that tightly bind the virus and prevent mucosal translocation might prevent in vivo infection, even if they lack in vitro neutralizing activity. sIgA antibodies would be particularly desirable in this context, as the secretory component of the antibody specifically binds mucus94. Developing a safe and effective strategy for inducing durable sIgA responses in the genital tract of women might be a worthy goal for future research. Other antibody-dependent mechanisms that might function to inhibit primary anogenital infection in vivo but would not be detected in standard in vitro neutralization assays include inhibition of HIV transcytosis across the epithelium, and Fc-mediated clearance of the virus by phagocytes86,92.
Like HPV, HSV has an inherently stable double-stranded DNA genome and would not be expected to rapidly evolve escape mutants in response to an effective vaccine. However, unlike HPV evolution, HSV evolution does not seem to have been driven by neutralizing antibody responses generated by naturally acquired HSV infections, as there are only two viral serotypes (and two corresponding viral genotypes). It has been argued that viruses which have evolved into many distinct serotypes, such as influenza virus and HPV, are more likely to be susceptible to antibody-mediated effector mechanisms, whereas viruses with few serotypes, such as HSV, are more likely to be controlled by cell-mediated immune responses95. However, passively transferred neutralizing antibodies can protect against experimental HSV infection in a mouse cervicovaginal-challenge model52. Thus, it is possible that pre-existing antibodies, perhaps at levels exceeding those induced by natural infection, would be protective in humans. However, in contrast to HPV, HSV has clearly evolved defence mechanisms to evade antibody-mediated inhibition, including inactivation of complement and blocking of Fc receptor-mediated clearance mechanisms. Vaccines that induce antibodies against the viral glycoproteins involved in these activities might have a higher effectiveness than the current prophylactic vaccines96,97. In addition, HSV can enter cells using several alternative cell surface receptors98. As a result, it may be difficult for vaccine-induced antibodies to simultaneously block enough of these interactions to consistently prevent entry. Accordingly, there has been limited success in human efficacy trials of subunit vaccines designed to induce antibody and TH cell responses to gB and gD, two HSV glycoproteins that are targets for neutralizing antibodies in in vitro assays99,100,101. Thus, it may be necessary to induce more potent and diverse antibodies, coupled with cell-mediated effector responses, at the site of initial infection to produce avaccine that effectively prevents sexual transmission of HSV.
Conclusions and future prospects
In this Review, a multifactorial explanation for the exceptional potency of HPV vaccines is presented. We posit that antibodies are likely to be the crucial effector mechanism for protection against HPV infection. The successful generation of antibodies is attributed to specific characteristics of the VLP antigen in the vaccine, and in particular to virus-like display of densely packed L1 epitopes, which are exceptionally well suited for inducing neutralizing antibody responses. We further argue that unique aspects of HPV biology, especially the prolonged infectious process in the target tissue, make HPV exceptionally susceptible to antibody-mediated inhibition. We have also attempted to apply the mechanistic insights underlying the success of HPV vaccines to the development of prophylactic vaccines for HIV and HSV, although a comprehensive presentation of the basic biology of HIV and HSV, and of the history of vaccine development for these viruses are beyond the scope of this Review. On the basis of the results of the HPV vaccine clinical trials, we predict that virus-like display could be effective at inducing antibody responses to other sexually transmitted viruses. However, the specific biology of these viruses might limit the ability of the induced antibodies to consistently prevent infection. In such cases, it might be more important to refine antibody specificity and maximize antibody avidity and titre. Nevertheless, we believe that the prevention of initial mucosal infection is currently the most promising approach to controlling the diseases caused by HIV and HSV. It remains to be determined whether this goal can be accomplished by potent antibody responses alone or whether it will require a combination of antibody- and cell-mediated effector mechanisms.

References
Fauci, A. S. & Morens, D. M. The perpetual challenge of infectious diseases. N. Engl. J. Med. 366, 454–461 (2012).
Giuliano, A. R. et al. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N. Engl. J. Med. 364, 401–411 (2011).
Herrero, R. et al. Prevention of persistent human papillomavirus infection by an HPV16/18 vaccine: a community-based randomized clinical trial in Guanacaste, Costa Rica. Cancer Discov. 1, 408–419 (2011).
Kjaer, S. K. et al. A pooled analysis of continued prophylactic efficacy of quadrivalent human papillomavirus (types 6/11/16/18) vaccine against high-grade cervical and external genital lesions. Cancer Prev. Res. (Phila.) 2, 868–878 (2009).
Lehtinen, M. et al. Overall efficacy of HPV-16/18 AS04-adjuvanted vaccine against grade 3 or greater cervical intraepithelial neoplasia: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 13, 89–99 (2011). End-of-study analyses of the Cervarix Phase III trial in young women.
Munoz, N. et al. Impact of human papillomavirus (HPV)-6/11/16/18 vaccine on all HPV-associated genital diseases in young women. J. Natl Cancer Inst. 102, 325–339 (2010). Pooled end-of-study analyses of the Gardasil Phase III trials in young women.
Palefsky, J. M. et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N. Engl. J. Med. 365, 1576–1585 (2011). The first study to demonstrate vaccine-mediated prevention of anal HPV infection and associated hyperproliferative diseases.
Bernard, H. U. et al. Classification of papillomaviruses (PVs) based on 189 PV types and proposal of taxonomic amendments. Virology 401, 70–79 (2010).
Munoz, N. et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 348, 518–527 (2003).
de Martel, C. et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol. 13, 607–615 (2012).
Parkin, D. M. The global health burden of infection-associated cancers in the year 2002. Int. J. Cancer 118, 3030–3044 (2006).
Peto, J., Gilham, C., Fletcher, O. & Matthews, F. E. The cervical cancer epidemic that screening has prevented in the UK. Lancet 364, 249–256 (2004).
Wu, X. et al. Human papillomavirus-associated cancers — United States, 2004–2008. Morb. Mortal. Wkly Rep. 61, 258–261 (2012).
Garland, S. M. et al. Natural history of genital warts: analysis of the placebo arm of 2 randomized phase III trials of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine. J. Infect. Dis. 199, 805–814 (2009).
Iftner, A. et al. The prevalence of human papillomavirus genotypes in nonmelanoma skin cancers of nonimmunosuppressed individuals identifies high-risk genital types as possible risk factors. Cancer Res. 63, 7515–7519 (2003).
Dürst, M., Gissmann, L., Ikenberg, H. & zur Hausen, H. A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions. Proc. Natl Acad. Sci. USA 80, 3812–3815 (1983).
McLaughlin-Drubin, M. E. & Munger, K. Oncogenic activities of human papillomaviruses. Virus Res. 143, 195–208 (2009).
Bosch, F. X., Lorincz, A., Munoz, N., Meijer, C. J. & Shah, K. V. The causal relation between human papillomavirus and cervical cancer. J. Clin. Pathol. 55, 244–265 (2002).
Bosch, F. X. et al. Epidemiology and natural history of human papillomavirus infections and type-specific implications in cervical neoplasia. Vaccine 26 (Suppl. 10), K1–K16 (2008).
Walboomers, J. M. et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 189, 12–19 (1999).
Hagensee, M. E., Yaegashi, N. & Galloway, D. A. Self-assembly of human papillomavirus type 1 capsids by expression of the L1 protein alone or by coexpression of the L1 and L2 capsid proteins. J. Virol. 67, 315–322 (1993).
Kirnbauer, R., Booy, F., Cheng, N., Lowy, D. R. & Schiller, J. T. Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc. Natl Acad. Sci. USA 89, 12180–12184 (1992). The initial report of self-assembly of L1 VLPs and their induction of high-titre neutralizing antibodies.
Rose, R. C., Bonnez, W., Reichman, R. C. & Garcea, R. L. Expression of human papillomavirus type 11 L1 protein in insect cells: in vivo and in vitro assembly of viruslike particles. J. Virol. 67, 1936–1944 (1993).
Einstein, M. H. et al. Comparison of the immunogenicity of the human papillomavirus (HPV)-16/18 vaccine and the HPV-6/11/16/18 vaccine for oncogenic non-vaccine types HPV-31 and HPV-45 in healthy women aged 18–45 years. Hum. Vaccin. 7, 1359–1373 (2011).
Joura, E. A. et al. HPV antibody levels and clinical efficacy following administration of a prophylactic quadrivalent HPV vaccine. Vaccine 26, 6844–6851 (2008).
Roteli-Martins, C. et al. Sustained immunogenicity and efficacy of the HPV-16/18 AS04-adjuvanted vaccine: up to 8.4 years of follow-up. Hum. Vaccin. Immunother. 8, 390–397 (2012).
Kreimer, A. R. et al. Proof-of-principle evaluation of the efficacy of fewer than three doses of a bivalent HPV16/18 vaccine. J. Natl Cancer Inst. 103, 1444–1451 (2011).
Kreimer, A. R. et al. Efficacy of a bivalent HPV 16/18 vaccine against anal HPV 16/18 infection among young women: a nested analysis within the Costa Rica Vaccine Trial. Lancet Oncol. 12, 862–870 (2011).
Brown, D. R. et al. The impact of quadrivalent human papillomavirus (HPV; types 6, 11, 16, and 18) L1 virus-like particle vaccine on infection and disease due to oncogenic nonvaccine HPV types in generally HPV-naive women aged 16–26 years. J. Infect. Dis. 199, 926–935 (2009).
Wheeler, C. M. et al. Cross-protective efficacy of HPV-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by non-vaccine oncogenic HPV types: 4-year end-of-study analysis of the randomised, double-blind PATRICIA trial. Lancet Oncol. 13, 100–110 (2011).
The FUTURE II Study Group. Quadrivalent vaccine against human papillomavirus to prevent high-grade cervical lesions. N. Engl. J. Med. 356, 1915–1927 (2007).
Hildesheim, A. et al. Effect of human papillomavirus 16/18 L1 viruslike particle vaccine among young women with preexisting infection: a randomized trial. JAMA 298, 743–753 (2007).
Joura, E. A. et al. Effect of the human papillomavirus (HPV) quadrivalent vaccine in a subgroup of women with cervical and vulvar disease: retrospective pooled analysis of trial data. BMJ 344, e1401 (2012).
Brotherton, J. M. et al. Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study. Lancet 377, 2085–2092 (2011). The first indication of the effectiveness of an HPV vaccine against cervical dysplasia in a general vaccination programme.
Donovan, B. et al. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: analysis of national sentinel surveillance data. Lancet Infect. Dis. 11, 39–44 (2011).
Roden, R. B. S. et al. In vitro generation and type-specific neutralization of a human papillomavirus type 16 virion pseudotype. J. Virol. 70, 5875–5883 (1996).
Romanowski, B. et al. Sustained efficacy and immunogenicity of the human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine: analysis of a randomised placebo-controlled trial up to 6.4 years. Lancet 374, 1975–1985 (2009).
Pastrana, D. V. et al. Reactivity of human sera in a sensitive, high-throughput pseudovirus-based papillomavirus neutralization assay for HPV16 and HPV18. Virology 321, 205–216 (2004).
Breitburd, F. et al. Immunization with virus-like particles from cottontail rabbit papillomavirus (CRPV) can protect against experimental CRPV infection. J. Virol. 69, 3959–3963 (1995).
Suzich, J. A. et al. Systemic immunization with papillomavirus L1 protein completely prevents the development of viral mucosal papillomas. Proc. Natl Acad. Sci. USA 92, 11553–11557 (1995).
Roberts, J. N. et al. Genital transmission of HPV in a mouse model is potentiated by nonoxynol-9 and inhibited by carrageenan. Nature Med. 13, 857–861 (2007).
Longet, S., Schiller, J. T., Bobst, M., Jichlinski, P. & Nardelli-Haefliger, D. A. Murine genital-challenge model is a sensitive measure of protective antibodies against human papillomavirus infection. J. Virol. 85, 13253–13259 (2011).
Kemp, T. J. et al. HPV16/18 L1 VLP vaccine induces cross-neutralizing antibodies that may mediate cross-protection. Vaccine 29, 2011–2014 (2011).
Giannini, S. L. et al. Enhanced humoral and memory B cellular immunity using HPV16/18 L1 VLP vaccine formulated with the MPL/aluminium salt combination (AS04) compared to aluminium salt only. Vaccine 24, 5937–5949 (2006).
Tobery, T. W. et al. Effect of vaccine delivery system on the induction of HPV16L1-specific humoral and cell-mediated immune responses in immunized rhesus macaques. Vaccine 21, 1539–1547 (2003).
De Bruijn, M. L. H. et al. L1-specific protection from tumor challenge elicited by HPV16 virus-like particles. Virology 250, 371–376 (1998).
Doorbar, J. The papillomavirus life cycle. J. Clin. Virol. 32 (Suppl. 1), S7–S15 (2005).
Block, S. L. et al. Comparison of the immunogenicity and reactogenicity of a prophylactic quadrivalent human papillomavirus (types 6, 11, 16, and 18) L1 virus-like particle vaccine in male and female adolescents and young adult women. Pediatrics 118, 2135–2145 (2006).
Pedersen, C. et al. Immunization of early adolescent females with human papillomavirus type 16 and 18 L1 virus-like particle vaccine containing AS04 adjuvant. J. Adolesc. Health 40, 564–571 (2007).
Petaja, T. et al. Immunogenicity and safety of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine in healthy boys aged 10–18 years. J. Adolesc. Health 44, 33–40 (2009).
Mestecky, J., Raska, M., Novak, J., Alexander, R. C. & Moldoveanu, Z. Antibody-mediated protection and the mucosal immune system of the genital tract: relevance to vaccine design. J. Reprod. Immunol. 85, 81–85 (2010).
Li, Z. et al. Transfer of IgG in the female genital tract by MHC class I-related neonatal Fc receptor (FcRn) confers protective immunity to vaginal infection. Proc. Natl Acad. Sci. USA 108, 4388–4393 (2011).
Nardelli-Haefliger, D. et al. Specific antibody levels at the cervix during the menstrual cycle of women vaccinated with human papillomavirus 16 virus-like particles. J. Natl Cancer Inst. 95, 1128–1137 (2003).
Trus, B. L. et al. Novel structural features of bovine papillomavirus capsid revealed by a three dimensional reconstruction to 9Å resolution. Nature Struct. Biol. 4, 413–420 (1997).
Bachmann, M. F. et al. The influence of antigen organization on B cell responsiveness. Science 262, 1448–1451 (1993).
Jennings, G. T. & Bachmann, M. F. The coming of age of virus-like particle vaccines. Biol. Chem. 389, 521–536 (2008).
Chackerian, B., Lenz, P., Lowy, D. R. & Schiller, J. T. Determinants of autoantibody induction by conjugated papillomavirus virus-like particles. J. Immunol. 169, 6120–6126 (2002).
Einstein, M. H. et al. Comparison of the immunogenicity and safety of Cervarix and Gardasil human papillomavirus (HPV) cervical cancer vaccines in healthy women aged 18–45 years. Hum. Vaccin. 5, 705–719 (2009).
Harro, C. D. et al. Safety and immunogenicity trial in adult volunteers of a human papillomavirus 16 L1 virus-like particle vaccine. J. Natl Cancer Inst. 93, 284–292 (2001).
Amanna, I. J. & Slifka, M. K. Mechanisms that determine plasma cell lifespan and the duration of humoral immunity. Immunol. Rev. 236, 125–138 (2010).
Amanna, I. J., Carlson, N. E. & Slifka, M. K. Duration of humoral immunity to common viral and vaccine antigens. N. Engl. J. Med. 357, 1903–1915 (2007). A study which provides compelling evidence that viral vaccines can induce durable antibody responses to virion surface elements.
Lenz, P., Lowy, D. R. & Schiller, J. T. Papillomavirus virus-like particles induce cytokines characteristic of innate immune responses in plasmacytoid dendritic cells. Eur. J. Immunol. 35, 1548–1556 (2005).
Lenz, P. et al. Interaction of papillomavirus virus-like particles with human myeloid antigen-presenting cells. Clin. Immunol. 106, 231–237 (2003).
Lin, Y.-L., Borenstein, L. A., Selvakumar, R., Ahmed, R. & Wettstein, F. O. Effective vaccination against papilloma development by immunization with L1 or L2 structural protein of cottontail rabbit papillomavirus. Virology 187, 612–619 (1992).
Carter, J. J. et al. Identification of human papillomavirus type 16 L1 surface loops required for neutralization by human sera. J. Virol. 80, 4664–4672 (2006).
Pastrana, D. V., Vass, W. C., Lowy, D. R. & Schiller, J. T. NHPV16 VLP vaccine induces human antibodies that neutralize divergent variants of HPV16. Virology 279, 361–369 (2001).
Bernard, H. U., Calleja-Macias, I. E. & Dunn, S. T. Genome variation of human papillomavirus types: phylogenetic and medical implications. Int. J. Cancer 118, 1071–1076 (2006).
Chan, S.-Y. et al. Molecular variants of human papillomaviru-16 from four continents suggest pandemic spread of the virus and its coevolution with humankind. J. Virol. 66, 2057–2066 (1992).
Kines, R. C., Thompson, C. D., Lowy, D. R., Schiller, J. T. & Day, P. M. The initial steps leading to papillomavirus infection occur on the basement membrane prior to cell surface binding. Proc. Natl Acad. Sci. USA 106, 20458–20463 (2009). This article describes the unique mechanism of HPV infection of cervicovaginal tissue in vivo.
Day, P. M. et al. In vivo mechanisms of vaccine-induced protection against HPV infection. Cell Host Microbe 8, 260–270 (2010). This report documents the mechanisms by which VLP antibodies can prevent cervicovaginal HPV infection.
Stanley, M. Immunobiology of HPV and HPV vaccines. Gynecol. Oncol. 109, S15–S21 (2008).
Carter, J. J. et al. Comparison of human papillomavirus types 16, 18, and 6 capsid antibody responses following incident infection. J. Infect. Dis. 181, 1911–1919 (2000).
Liaw, K. L. et al. A prospective study of human papillomavirus (HPV) type 16 DNA detection by polymerase chain reaction and its association with acquisition and persistence of other HPV types. J. Infect. Dis. 183, 8–15 (2001).
Plummer, M., Schiffman, M., Castle, P. E., Maucort-Boulch, D. & Wheeler, C. M. A 2-year prospective study of human papillomavirus persistence among women with a cytological diagnosis of atypical squamous cells of undetermined significance or low-grade squamous intraepithelial lesion. J. Infect. Dis. 195, 1582–1589 (2007).
Chaturvedi, A. K. et al. Human papillomavirus infection with multiple types: pattern of coinfection and risk of cervical disease. J. Infect. Dis. 203, 910–920 (2011).
Kjaer, S. K., Frederiksen, K., Munk, C. & Iftner, T. Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: role of persistence. J. Natl Cancer Inst. 102, 1478–1488 (2010).
Girard, M. P. & Plotkin, S. A. HIV vaccine development at the turn of the 21st century. Curr. Opin. HIV AIDS 7, 4–9 (2012).
Johnston, C., Koelle, D. M. & Wald, A. HSV-2: in pursuit of a vaccine. J. Clin. Invest. 121, 4600–4609 (2011).
Buonaguro, L., Tagliamonte, M., Tornesello, M. L. & Buonaguro, F. M. Developments in virus-like particle-based vaccines for infectious diseases and cancer. Expert Rev. Vaccines 10, 1569–1583 (2011).
Zhu, P. et al. Distribution and three-dimensional structure of AIDS virus envelope spikes. Nature 441, 847–852 (2006).
Bomsel, M. et al. Immunization with HIV-1 gp41 subunit virosomes induces mucosal antibodies protecting nonhuman primates against vaginal SHIV challenges. Immunity 34, 269–280 (2011).
Kaushic, C., Nazli, A., Ferreira, V. H. & Kafka, J. K. Primary human epithelial cell culture system for studying interactions between female upper genital tract and sexually transmitted viruses, HSV-2 and HIV-1. Methods 55, 114–121 (2011).
Hladik, F. & Hope, T. J. HIV infection of the genital mucosa in women. Curr. HIV/AIDS Rep. 6, 20–28 (2009).
Pantophlet, R., Wang, M., Aguilar-Sino, R. O. & Burton, D. R. The human immunodeficiency virus type 1 envelope spike of primary viruses can suppress antibody access to variable regions. J. Virol. 83, 1649–1659 (2009).
Wei, X. et al. Antibody neutralization and escape by HIV-1. Nature 422, 307–312 (2003).
Mascola, J. R. & Montefiori, D. C. The role of antibodies in HIV vaccines. Annu. Rev. Immunol. 28, 413–444 (2010).
Mascola, J. R. et al. Protection of macaques against vaginal transmission of a pathogenic HIV-1/SIV chimeric virus by passive infusion of neutralizing antibodies. Nature Med. 6, 207–210 (2000).
Powers, K. A., Poole, C., Pettifor, A. E. & Cohen, M. S. Rethinking the heterosexual infectivity of HIV-1: a systematic review and meta-analysis. Lancet Infect. Dis. 8, 553–563 (2008).
Keele, B. F. et al. Identification and characterization of transmitted and early founder virus envelopes in primary HIV-1 infection. Proc. Natl Acad. Sci. USA 105, 7552–7557 (2008).
Burchell, A. N., Coutlee, F., Tellier, P. P., Hanley, J. & Franco, E. L. Genital transmission of human papillomavirus in recently formed heterosexual couples. J. Infect. Dis. 204, 1723–1729 (2011).
Rerks-Ngarm, S. et al. Vaccination with ALVAC and AIDSVAX to prevent HIV-1 infection in Thailand. N. Engl. J. Med. 361, 2209–2220 (2009).
Tomaras, G. D. & Haynes, B. F. Strategies for eliciting HIV-1 inhibitory antibodies. Curr. Opin. HIV AIDS 5, 421–427 (2010).
Lai, S. K. et al. Human immunodeficiency virus type 1 is trapped by acidic but not by neutralized human cervicovaginal mucus. J. Virol. 83, 11196–11200 (2009).
Phalipon, A. et al. Secretory component: a new role in secretory IgA-mediated immune exclusion in vivo. Immunity 17, 107–115 (2002).
Bachmann, M. F. & Zinkernagel, R. M. The influence of virus structure on antibody responses and virus serotype formation. Immun. Today 17, 553–558 (1996).
Awasthi, S., Lubinski, J. M. & Friedman, H. M. Immunization with HSV-1 glycoprotein C prevents immune evasion from complement and enhances the efficacy of an HSV-1 glycoprotein D subunit vaccine. Vaccine 27, 6845–6853 (2009).
Hook, L. M., Huang, J., Jiang, M., Hodinka, R. & Friedman, H. M. Blocking antibody access to neutralizing domains on glycoproteins involved in entry as a novel mechanism of immune evasion by herpes simplex virus type 1 glycoproteins C and E. J. Virol. 82, 6935–6941 (2008).
Karasneh, G. A. & Shukla, D. Herpes simplex virus infects most cell types in vitro: clues to its success. Virol. J. 8, 481 (2011).
Corey, L. et al. Recombinant glycoprotein vaccine for the prevention of genital HSV-2 infection: two randomized controlled trials. JAMA 282, 331–340 (1999).
Stanberry, L. R. et al. Glycoprotein-D-adjuvant vaccine to prevent genital herpes. N. Engl. J. Med. 347, 1652–1661 (2002).
Belshe, R. B. et al. Efficacy results of a trial of a herpes simplex vaccine. N. Engl. J. Med. 366, 34–43 (2012).
Buck, C. B., Pastrana, D. V., Lowy, D. R. & Schiller, J. T. Efficient intracellular assembly of papillomaviral vectors. J. Virol. 78, 751–757 (2004).
Acknowledgements
The authors' research was supported by the Intramural Research Program, Center for Cancer Research, National Cancer Institute, US National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
John T. Schiller and Douglas R. Lowy are inventors on US Government-owned patents that have been licensed to Merck and GlaxoSmithKine Biologicals, the two companies that market human papillomavirus vaccines.
Related links
Glossary
- Hyperproliferative diseases
-
Pathologies that are characterized by excessive cell growth.
- Stratified squamous epithelium
-
Multilayered body surface tissue in which the cells undergo an ordered process of differentiation after they divide and lose their attachment to the basement membrane. The cells of the uppermost layers acquire a flattened appearance.
- Benign epithelial hyperplasia
-
A focal abnormal proliferation of epithelial cells, with no invasion of surrounding tissues.
- Mucosatropic
-
Having an affinity for mucosal epithelium.
- Intraepithelial neoplasia
-
A histology term denoting a focus of abnormally proliferating cells within an epithelium. Also called dysplasia.
- Adjuvant
-
A substance that increases the immune response to a vaccine.
- Sterilizing immunity
-
An immune response that prevents initial infection in addition to preventing the disease outcome.
- Breakthrough infections
-
Infections that occur despite preventive measures.
- Herd immunity
-
The protection of non-vaccinated individuals in a population as a result of the overall reduction in microbial prevalence and, thereby, transmission to individuals who remain susceptible to infection.
- Immunobridging studies
-
Vaccine trials that measure immune response outcomes and can be used to extend vaccination recommendations to groups for which vaccine efficacy against the disease has not been formally demonstrated.
- Transudation
-
The transport of plasma-derived antibodies across an intact epithelium.
- Fc receptor
-
A cell surface molecule that binds a constant-region (Fc) domain of an antibody.
- Exudation
-
The passive leakage of plasma components at a site where the barrier function of an epithelial tissue has been compromised.
- Pap test
-
(Papanicolaou test). A test for the detection of cervical cancer and pre-cancerous lesions. The test involves the collection of superficial cervical epithelial cells, staining of these cells and microscopic detection of abnormal cells.
- Central self-antigens
-
Components of the body (self) that are regularly exposed to the systemic immune system.
- Seroconversion
-
A change from having undetectable levels to having detectable levels of serum antibodies against a specific antigen.
- Transcytosis
-
Active transport of an infectious virion across an intact epithelium.
- Complement
-
A complex set of plasma proteins that act together to inactivate extracellular microorganisms.
Rights and permissions
About this article
Cite this article
Schiller, J., Lowy, D. Understanding and learning from the success of prophylactic human papillomavirus vaccines. Nat Rev Microbiol 10, 681–692 (2012). https://doi.org/10.1038/nrmicro2872
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrmicro2872
