
Abstract
Background
Although a number of robot-assisted minimally invasive esophagectomy (RAMIE) procedures have been performed due to three-dimensional field of view, image stabilization, and flexible joint function, both the surgeons and surgical teams require proficiency. This study aimed to establish an artificial intelligence (AI)-based automated surgical-phase recognition system for RAMIE by analyzing robotic surgical videos.
Methods
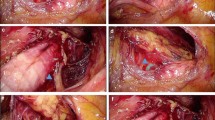
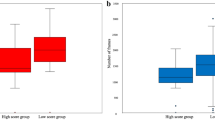
This study enrolled 31 patients who underwent RAMIE. The videos were annotated into the following nine surgical phases: preparation, lower mediastinal dissection, upper mediastinal dissection, azygos vein division, subcarinal lymph node dissection (LND), right recurrent laryngeal nerve (RLN) LND, left RLN LND, esophageal transection, and post-dissection to completion of surgery to train the AI for automated phase recognition. An additional phase (“no step”) was used to indicate video sequences upon removal of the camera from the thoracic cavity. All the patients were divided into two groups, namely, early period (20 patients) and late period (11 patients), after which the relationship between the surgical-phase duration and the surgical periods was assessed.
Results
Fourfold cross validation was applied to evaluate the performance of the current model. The AI had an accuracy of 84%. The preparation (p = 0.012), post-dissection to completion of surgery (p = 0.003), and “no step” (p < 0.001) phases predicted by the AI were significantly shorter in the late period than in the early period.
Conclusions
A highly accurate automated surgical-phase recognition system for RAMIE was established using deep learning. Specific phase durations were significantly associated with the surgical period at the authors’ institution.



Similar content being viewed by others

References
Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
Kitagawa Y, Uno T, Oyama T, et al. Esophageal cancer practice guidelines 2017 edited by the Japan Esophageal Society: part 1. Esophagus. 2019;16:1–24.
Straatman J, Van Der Wielen N, Cuesta MA, et al. Minimally invasive versus open esophageal resection: three-year follow-up of the previously reported randomized controlled trial: the TIME trial. Ann Surg. 2017;266:232–6.
Kataoka K, Takeuchi H, Mizusawa J, et al. A randomized phase III trial of thoracoscopic versus open esophagectomy for thoracic esophageal cancer: Japan Clinical Oncology Group Study (JCOG) 1409. Jpn J Clin Oncol. 2016;46:174–7.
Kernstine KH. The first series of completely robotic esophagectomies with three-field lymphadenectomy: initial experience. Surg Endosc Other Interv Tech. 2008;22:2102.
Park SY, Kim DJ, Yu WS, Jung HS. Robot-assisted thoracoscopic esophagectomy with extensive mediastinal lymphadenectomy: experience with 114 consecutive patients with intrathoracic esophageal cancer. Dis Esophagus. 2016;29:326–32.
van der Sluis PC, Ruurda JP, Verhage RJJ, et al. Oncologic long-term results of robot-assisted minimally invasive thoraco-laparoscopic esophagectomy with two-field lymphadenectomy for esophageal cancer. Ann Surg Oncol. 2015;22:S1350–6. https://doi.org/10.1245/s10434-015-4544-x.
Luketich JD, Pennathur A, Awais O, et al. Outcomes after minimally invasive esophagectomy: review of over 1000 patients. Ann Surg. 2012;256:95–103.
Suda K, Ishida Y, Kawamura Y, et al. Robot-assisted thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve for esophageal squamous cell carcinoma in the prone position: technical report and short-term outcomes. World J Surg. 2012;36:1608–16.
Morimoto Y, Kawakubo H, Ishikawa A, et al. Short-term outcomes of robot-assisted minimally invasive esophagectomy with extended lymphadenectomy for esophageal cancer compared with video-assisted minimally invasive esophagectomy: a single-center retrospective study. Asian J Endosc Surg. 2021;15:270–8.
van der Sluis PC, van der Horst S, May AM, et al. Robot-assisted minimally invasive thoracolaparoscopic esophagectomy versus open transthoracic esophagectomy for resectable esophageal cancer: a randomized controlled trial. Ann Surg. 2019;269:621–30.
Tagkalos E, van der Sluis PC, Berlth F, et al. Robot-assisted minimally invasive thoraco-laparoscopic esophagectomy versus minimally invasive esophagectomy for resectable esophageal adenocarcinoma, a randomized controlled trial (ROBOT-2 trial). BMC Cancer. 2021;21:1060.
Chao YK, Li ZG, Wen YW, et al. Robotic-assisted esophagectomy vs video-assisted thoracoscopic esophagectomy (REVATE): study protocol for a randomized controlled trial. Trials. 2019;20:1–8.
Esteva A, Kuprel B, Novoa RA, et al. Dermatologist-level classification of skin cancer with deep neural networks. Nature. 2017;542:115–8.
Misawa M, Kudo SE, Mori Y, et al. Artificial intelligence-assisted polyp detection for colonoscopy: initial experience. Gastroenterology. 2018;154:2027-29.e3.
Hirasawa T, Aoyama K, Tanimoto T, et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer. 2018;21:653–60.
Zhao W, Yang J, Sun Y, et al. 3D deep learning from CT scans predicts tumor invasiveness of subcentimeter pulmonary adenocarcinomas. Cancer Res. 2018;78:6881–9.
Takeuchi M, Seto T, Hashimoto M, et al. Performance of a deep learning-based identification system for esophageal cancer from CT images. Esophagus. 2021;18:612–20.
Garrow CR, Kowalewski KF, Li L, et al. Machine learning for surgical phase recognition: a systematic review. Ann Surg. 2021;273:684–93.
Bodenstedt S, Wagner M, Katić D, et al. Unsupervised temporal context learning using convolutional neural networks for laparoscopic workflow analysis. Retrieved 20 April 2022 at http://arxiv.org/abs/1702.03684.
Padoy N, Blum T, Ahmadi SA, Feussner H, Berger MO, Navab N. Statistical modeling and recognition of surgical workflow. Med Image Anal. 2012;16:632–41.
Guédon ACP, Meij SEP, Osman KNMMH, et al. Deep learning for surgical phase recognition using endoscopic videos. Surg Endosc. 2021;35:6150–7.
Hashimoto DA, Rosman G, Witkowski ER, et al. Computer vision analysis of intraoperative video: automated recognition of operative steps in laparoscopic sleeve gastrectomy. Ann Surg. 2019;270:414–21.
Kitaguchi D, Takeshita N, Matsuzaki H, et al. Automated laparoscopic colorectal surgery workflow recognition using artificial intelligence: experimental research. Int J Surg. 2020;79:88–94.
Rice TW, Patil DT, Blackstone EH. 8th Edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: application to clinical practice. Ann Cardiothorac Surg. 2017;6:119–30.
Czempiel T, Paschali M, Keicher M, et al. TeCNO: surgical-phase recognition with multi-stage temporal convolutional networks. Lect Notes Comput Sci LNCS. 2020;12263:343–52.
Hernandez JM, Dimou F, Weber J, et al. Defining the learning curve for robotic-assisted esophagogastrectomy. J Gastrointest Surg. 2013;17:1346–51.
Park SY, Kim DJ, Kang DR, Haam SJ. Learning curve for robotic esophagectomy and dissection of bilateral recurrent laryngeal nerve nodes for esophageal cancer. Dis Esophagus. 2017;30:1–9.
Ward TM, Hashimoto DA, Ban Y, et al. Automated operative phase identification in peroral endoscopic myotomy. Surg Endosc. 2021;35:4008–15.
Kitaguchi D, Takeshita N, Matsuzaki H, et al. Deep learning-based automatic surgical step recognition in intraoperative videos for transanal total mesorectal excision. Surg Endosc. 2022;36:1143–51.
Levin M, McKechnie T, Khalid S, Grantcharov TP, Goldenberg M. Automated methods of technical skill assessment in surgery: a systematic review. J Surg Educ. 2019;76:1629–39.
Acknowledgment
We thank Kumiko Motooka, a staff member at the Department of Surgery in Keio University School of Medicine, for her help with the preparation of this report.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Yuko Kitagawa received lecture fees from Chugai Pharmaceutical Co., Ltd., Taiho Pharmaceutical Co., Ltd, Asahi Kasei Pharma Corporation, Otsuka Pharmaceutical Factory, Inc., Shionogi & Co., Ltd., Nippon Covidien, Inc., Ono Pharmaceutical Co., Ltd., and Bristol-Myers Squibb K.K. Yuko Kitagawa was supported by grants from Chugai Pharmaceutical Co., Ltd., Taiho Pharmaceutical Co., Ltd, Yakult Honsha Co. Ltd., Asahi Kasei Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Tsumura & Co., Kyouwa Hakkou Kirin Co., Ltd., Dainippon Sumitomo Pharma Co., Ltd., EA Pharma Co., Ltd., Astellas Pharma, Inc., Toyama Chemical Co., Ltd., Medicon, Inc., Kaken Pharmaceutical Co. Ltd., Eisai Co., Ltd., Otsuka Pharmaceutical Factory, Inc., Teijin Pharma Limited, Nihon Pharmaceutical Co., Ltd., and Nippon Covidien, Inc. Yuko Kitagawa held an endowed chair provided by Chugai Pharmaceutical Co., Ltd. and Taiho Pharmaceutical Co., Ltd, outside the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Takeuchi, M., Kawakubo, H., Saito, K. et al. Automated Surgical-Phase Recognition for Robot-Assisted Minimally Invasive Esophagectomy Using Artificial Intelligence. Ann Surg Oncol 29, 6847–6855 (2022). https://doi.org/10.1245/s10434-022-11996-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-11996-1